OPIOID CRISIS DEATHS ARE RISING IN A RURAL WASHINGTON COUNTY – ANOTHER EXCEPTION PROVING THE LETHAL RULE
In Grant County, medical opioid cures have been as accessible as elsewhere in the U.S., but not life-saving naloxone
by Clark Miller
Published February 20, 2026
Readers who have been following posts here at A Critical Discourse or at Illness and Cure will be familiar with that “lethal rule“. (and here). The ostensible exceptions to the general trend, or “rule” are states and locales where, unlike in most of the rest of the U.S., opioid overdose deaths did not begin to drop in late 2023, give or take some months, instead earlier or later. Or didn’t drop, or increased.
In fact, the temporal course of opioid OD death trends has varied wildly across varied and disparate states and locales, with no general patterns discernible.
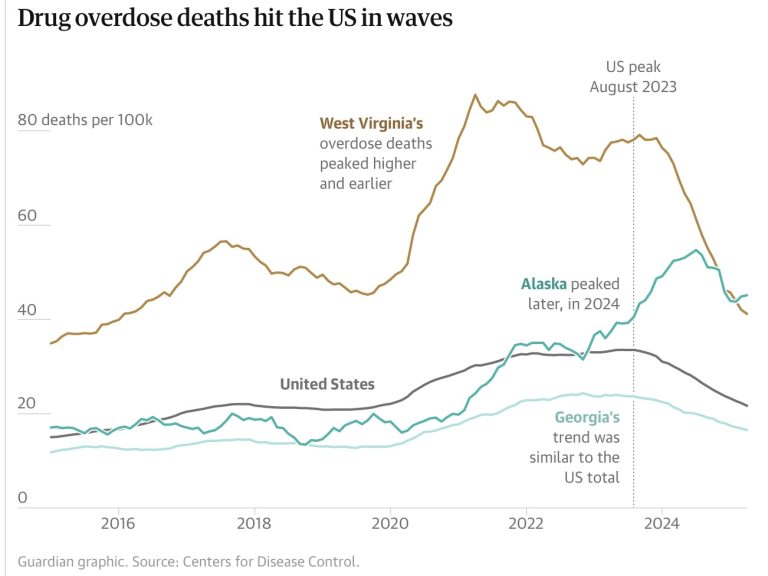
Except for this pattern, which holds consistently and is described in this recent post that deconstructs an “exclusive analysis” in The Guardian.
From that November, 2025 post at ACD –
What is entirely clear is that your benighted experts and science reporters have no idea how to make sense of trends like those.
But we do, and there’s nothing mysterious about it.
All we have to do is look at the wealth of data and evidence for diverse locales, readily available and omitted from The Guardian’s Exclusive Analysis.
The trend and its causes are clear for West Virginia.

And for Alaska –
But those aren’t the only cases. Instead, consistently in every state and locale examined, the causal relationship holds between timing and effectiveness of naloxone campaigns and drops in incidence of fatal opioid overdoses –
Let’s repeat that: even as increasingly effective naloxone campaigns are moderating incidence of fatal overdose, the high-risk opioid use desperately necessitating those intensive, nearly nation-wide campaigns is increasing.
It’s the situation not just in Columbus Ohio, but everywhere, evidenced in diverse states, cities and locales across the U.S. consistently, wherever data is available for analysis.
But not in locations that are the exceptions that prove that lethal rule, where overdose deaths did not decrease or increased while almost all other states saw sigificant drops, excpetions like Nevada, where lack of effective naloxone distribution and use, along with reckless dispensing of the common street currency for fentanyl (also known as buprenorphine, the “proven” medical cure for opioid use) combine to keep opioid OD deaths mounting. And locations like Iowa and South Dakota, for the same reasons.
The lethal rule is also proven by the exception San Francisco, where an intensive, successful naloxone campaign finally dropped opioid fatal ODs, lagging other locales, followed by opioid deaths now rising again predictably with intensive, publicly-funded dispensing under the direction of medical addiction treatment experts of that common street currency for fentanyl, “bupe, subs”, also in demand for “bridging” or “chipping” to enable fentanyl’s (or heroin’s) episodic use.
Back to our current post and to what’s been going on in Grant County, Washington, located east of the Cascades, north of the Columbia, in sparsely populated high desert.
But not very isolated or remote, a reasonable drive from the sizeable cities of Yakima and Spokane.

Even without that proximity to cities with residential treatment facilities (“rehab” programs), it is would not be possible to seriously consider the rationalizations of county officials that lack of access to expert gold standard treatment explains the persistent increases in deaths by high-risk opioid use.
We’ll get to that soon, but first –

GRANT COUNTY — Grant County recorded a record number of overdose deaths in 2025, according to data released by the Grant County Coroner’s Office.
The county reported 38 overdose deaths last year, marking an increase of four compared to the previous year. Most of the deaths were linked to fentanyl and methamphetamine, while other cases involved cocaine or a combination of multiple substances. …
The health district says it will continue working with medical providers and community partners to address gaps in treatment and expand overdose prevention efforts as the crisis continues to evolve.
That’s not a huge increase, 4 fentanyl deaths, but in Grant County it is: about an 11 percent increase, and in any case, not a decrease in opioid deaths like just about everywhere else in the U.S.
So Grant County really is an anomaly … until we take the time to take a look at what’s been happening, and not happening there, then we’ll see it fits, as every other locale has, the pattern, the lethal rule.
But what about treatment? Is it inaccessible to Grant County residents?
Clearly, it is not.
Here’s why.
America’s top experts and media have been reminding us over decades – as deaths have mounted – that these are stand-alone medications, without the need for talk therapies or other supports, so that attending therapy sessions or other programming is not needed, in fact may constitute barriers to use of the proven medical cures.
If you’re in Grant County and engaged in compulsive, high-risk opioid use, and are challenged by material and/or financial security, then access to Washington state’s Medicaid coverage would have paid for any and all services and prescriptions.
Even likely pay for transport to Yakima or Spokane if you decided to take advantage of the newest, “game changing“, fail-safe buprenorphine formulation – injectable 30-day Sublocade, requiring travel to appointments only once every 30 days.
Or to travel to one of those cities to be prescribed buprenorphine or methadone at one of the numerous state-recognized “opioid treatment programs” in Spokane or Yakima. Washington was one of the majority of states responding to COVID conditions in 2020 by relaxing longstanding methadone take-home rules, so daily visits to a methadone clinic in one of those cities would not have been required over past years for a Grant County resident.
But in any case and in addition to those options, the life-saving medication Suboxone would have been easily available to you, and cheap, on the streets, where for decades it has been one of the most available drugs in economies of illicit opioid and other drug use. It’s everywhere, and the rationalization that America’s expert opioid treatments are in short supply or hard to access is simply a lie (and here).
Think about it just a minute. If you’re trapped in high-risk fentanyl use, at some risk of death each day, and miserable, wouldn’t you get help accessing resources to get to one of those opioid treatment programs once a week? Or once a month for Sublocade injections? If that’s all it takes to save your life?
Or, as an experienced illicit opioid user, simply ask around and start buying, instead of fentanyl, the cheap, easily available, safe (packaged) buprenorphine, understood universally by experts as the proven, life-saving medication that would cure your opioid addition without you committing to additional forms of treatment?
And if you believe it actually works?
See how easy that was? To point out and dismantle the lethal lies you’ve been provided for decades?
So, it’s not about treatment. What else could it be?
Let’s take a look.
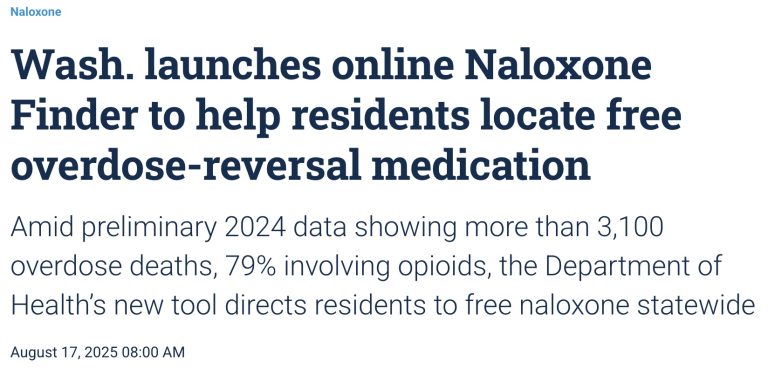
OLYMPIA, Wash. — The Washington State Department of Health has unveiled an online tool designed to help residents swiftly locate free naloxone, a medication that can reverse opioid overdoses, including those related to fentanyl.
The only place for residents in both Grant and Adams Counties to get free naloxone is the Grant County Health District, 1038 Ivy Ave. in Moses Lake. There are no locations in Adams County.
(emphasis added)
Okay, reality check:
That is a local news piece for Grant County.
It was published August 17, 2025.
Part of the report states that at the time of that report and as the state was rolling out an online guide for residents to access naloxone, “The only place for residents in both Grant and Adams Counties to get free naloxone is the Grant County Health District“…
There’s more.
“Grant County Health District made it accessible for free because there was some controversy for the community,” Communications Specialist Elaine Rodriguez said. “I guess for us, we realized that it worked out for us in our end, to just keep it subtle, but also very accessible and very private for someone to pick it up right there in front of the entrance of the health district office.”
Huh?
In mid-2025, with opioid deaths increasing, and “there was some controversy” in the community about provision of life-saving naloxone? And it’s distribution has needed to be “subtle”? And for individuals fearful of stigmatization, picking it up “right there in front of the entrance to the health district office” is “very private”?
That sounds quite different from the successful, well-funded, targeted, intensive, successful naloxone provision campaigns that have been in full force for years across much of the country. Including in very small, rural communities.
That sounds like an abject failure to provide the only intervention saving lives by reversing potentially fatal opioid overdoses.
But there’s more.
“There are not a lot of places that have the accessibility,” Rodriguez said. “We want to open that door for the community just in case for that person, or that loved one or anyone who may need Narcan.”
Okay … how do we interpret that?
“There are not a lot of places that have the accessibility,” Rodriguez said.
I guess not, just one in the county, mid-2025.
“We want to open that door for the community just in case for that person, or that loved one or anyone who may need Narcan.”
So ….apart from that “want”, there are plans? local organizations? county entities? anything resembling a program to get Narcan units where they could start saving lives?

There is no mystery here, no anomaly, no room to fabricate weak, evidence-free cover stories for America’s expert opioid treatment lethal failure.
Without the only, emergency intervention that has provided opioid crisis harm reduction, moderating lethal effects of gold standard treatments, increasing high-risk opioid use, overdoses, and deaths are predictable.
And with those desperate, emergency naloxone campaign reversals becoming routine, morphing into a new opioid crisis, things can only get worse.







