THE LETHAL ROLE OF ABDICATION OF THOUGHT IN A WORSENING OPIOID CRISIS
From all appearances and evidence, intellectual cowardice and impairment drive expert opioid crisis guidance and media messaging, lethally
by Clark Miller
Published April 24, 2026
Let’s start with a typical, corporate media account of changes in America’s opioid crisis, appearing recently.

There is a ray of hope in the opioid crisis that has claimed so many lives in southwestern Pennsylvania and across the nation: fatal overdoses have dramatically declined. …
According to county records, fatal overdoses began dropping just over two years ago. Overdoses suddenly fell from 665 in 2023 to 432 in 2024. So far, the preliminary number of deaths in 2025 shows an even further decline to 344.
The primary reason behind the drop appears to be the diminishing presence of the lethal drug fentanyl in the drug supply, which began disappearing after China bent to international pressure and clamped down on companies exporting the chemicals to make the drug.
That totally makes sense, doesn’t it?
Reinforced by a seminal report in one of America’s top journals of science, setting out the “supply shock” explanation for recent drops in opioid OD deaths elsewhere and generally.
So, that’s it, as reported in the news piece and on authority from the interviewed public health expert. Pretty sure that would be the explanation.
But let’s read on a bit further.
“It’s a relief,” said David Loveland of the Allegheny County Department of Human Services. “It’s been so distressing to see it rise for all those years. We’ve seen a 30 to 40 percent drop in fatal overdose rates here in Allegheny County.” …
“It appears they clamped down on them [on companies exporting fentanyl from China] about the exact same time that we saw the drop,” Loveland said. “And we do know the concentrations of fentanyl are going down. “
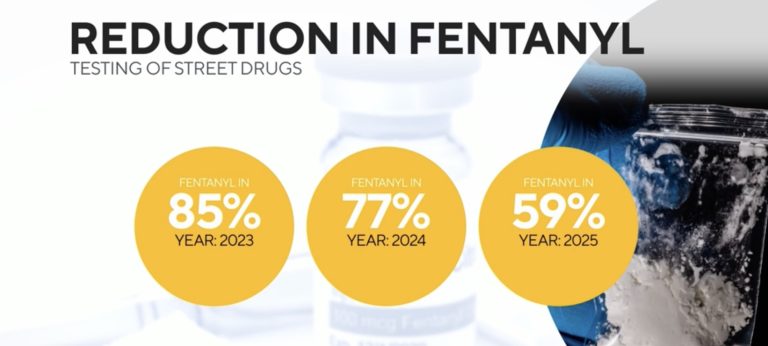
The organization Prevention Point Pittsburgh has quantified the reduction in fentanyl by sending samples of street drugs collected in Pittsburgh to the University of North Carolina for testing. Three years ago, they found fentanyl in 85 percent of the drugs sold. That fell to 77 percent in 2024. Last year, only 59 percent of the drugs sold as fentanyl actually contained the drug.
“In 2025, 40 percent of the samples we were seeing that are expected to be fentanyl contained no fentanyl or only a trace amount of fentanyl,” Alice Bell of Prevention Point Pittsburgh said.
Prevention Point also pioneered the distribution of the overdose reversal drug Naloxone, which is now readily available. Bell says less fentanyl and the use of Naloxone have resulted in a dramatic decrease in deaths, but says the danger isn’t over.
“The big concern with an unregulated drug supply is people do not know what they’re getting, and so if you have one batch that has a normal amount of fentanyl in it, we could see people dying,” Bell said.
[emphasis added]
Okay, wait … what!?
Let’s just unpack that before we move on. Not that it’s surprising, it’s what’s being reported everywhere: that faced with the persistent, uncontrolled variation, including in potency of the drug supply – affecting expectations and needs of high-risk users – those users don’t just stop using, instead keep using, seeking what they urgently need, even if they “do not know what they’re getting”. Of course they do. We’ll come back to this.
Okay, and … that’s just confusing, no longer clear even on the authority of public health experts and officials! Because it turns out there was a naloxone campaign involved at the same time, as in the rest of Pennsylvania. Now we have to think about things! Let’s come back to that too, it may be the least of factors driving the impairing confusion.
So, over the two years (2024 and 2025) of dramatically decreased fatal opioid overdoses in Pittsburgh (and Allegheny County), samples of street drugs (leaving aside the quite important questions about how representative those samples were of street drugs available to high-risk users) were found to be reduced in the percentage of those containing fentanyl, so “less fentanyl”, and “we do know the ocncentrations of fentanyl are going down“.
Okay. And?
Let’s actually think about some of this. Starting with:
“The big concern with an unregulated drug supply is people do not know what they’re getting, and so if you have one batch that has a normal amount of fentanyl in it, we could see people dying,” Bell said.
So,
“… the danger isn’t over”
and must not have been over during the recent years of variations in drug supply and dramatic opioid OD death reductions.
But how can that make sense?
Digression:
There is just one way, one way only, that naloxone (Narcan) can be effective to reduce opioid overdose deaths, and that is after a potentially fatal opioid overdose has occurred. At that point, it becomes remarkably effective, preventing, in a matter of minutes, an opioid overdose death from occurring.
All other conjectured factors employed to mystify recent, nationwide decreases in opioid deaths, including gold standard treatments and “supply shock” and other disruptions in availability or potency of drugs of abuse, are nearly the opposite in how – by the only possible means – they can have effects.
Clearly, not in the minutes after a potentially fatal opioid OD has occurred, but only by preventing those potentially fatal overdoses, meaning only by preventing high-risk opioid use.
So far so good?
So, how can that possibly make sense?
Make sense that high-risk users in Pittsburgh remained at high risk of opioid – fentanyl! – overdose and potentially death, while at the same time, variations in the street illicit opioid economy were leading to dramatic drops in fatal ODs? Which would, necessarily, have had to have been due to significant reductions in the behaviors of high-risk users, prevention of high-risk use in large numbers of high-risk users.
And? over the period of interest, while fentanyl, along with all kinds of other illicit and prescribed opioids and adulterants, were still there, available on the street to anyone determined to get them. Almost certainly, users encountered and experienced those variations in their daily use, and yet opioid overdose deaths dropped dramatically.
The interviewed social services worker was, of course, right, the danger wasn’t over, because there was no disruption of the desperate, driven need to use an unpredictable drug supply to gain relief from the overwhelmingly powerful inner states and drives that compel high-risk users to keep using, at high risk.
See how we did that? All it took was a few moments of thought, of healthy curiosity, of questioning.
We need to digress again.
Let’s imagine one of those high-risk fentanyl users, injecting or smoking what was just provided them as fentanyl.
Our user is feeling pretty dope sick and annoyed, but still level-headed, “guess I just need to get some more that those, crush em up and smoke some more of that weak shit”, or no, maybe go see dude in the park, I know they got tranq dope there, and H, and maybe even some different fettie, they all looked high af the other day. Anyway, there’s street benzos, I think that guy on 4th has good stuff”.
Our user pauses, visibly agitated, dope sick, but looking contemplative … continues … “yeah, yeah, there’s my man on the avenue, could share some of his methadone with me, owes me for all the times I shared mne with him, or subs, everywhere, still cheap, could bridge for a few days just I always do til I find the good dope agains in a few days. Suddenly our user, overwhelmed with despite all the options he has for getting high, and for “bridging” with widely available street suboxone for a few days while he finds “real dope”, makes a choice he’s never made before, over a decade of high-risk opioid use and uncertain supply, continuing in his thoughts, “Wait! … you know what? this is just too much damn trouble, I am just done … I am so done!
He makes his way to a detox program, then to rehab, then within a couple of months is in low-income housing, has a job, and never goes back to high-risk use of street opioids.
And because his story repeated itself hundreds of times in Allegheny County over the past two years, fatal opioid overdoses dropped.
Ha! Funny, right? Actually not, instead tragic, because that essentially never happens. What happens is what is reported to be happening in those street economies of illicit opioids and other drugs everywhere, every day.
Like in Arizona, where the known behaviors of high-risk opioid users are described in this recent post:
An independently nullifying deconstruction of opioid “supply shock” effects is outlined in the news piece we are considering.
Why is the opioid problem in Phoenix getting worse? One reason, Raminta Daniulaityte says, has to do with the stuff on the street.
Daniulaityte is a professor at Arizona State University’s College of Health Solutions. In June, she co-authored a study published in the International Journal of Drug Policy that examined Phoenix’s opioid crisis through the lens of fentanyl pills.
She interviewed drug users, the majority of whom said that fentanyl powder is known to be “significantly more dangerous” than illicitly manufactured fentanyl pills. Despite that, fentanyl powder has become more common on the street as the potency of the pills has waned.
“People are not getting what they need from (the pills),” Daniulaityte said.
That matches what the Arizona branch of the Drug Enforcement Administration has seen. In Arizona, the DEA saw a 79% increase in seizures of fentanyl powder between 2024 and 2025. Cheri Oz, the special agent who led the DEA’s Phoenix field office last year, said that many drug users are turning to powder to maintain their habit, leading to extreme variance in dosage.
Many participants in Daniulaityte’s study were aware of the dangers of fentanyl powder — “Almost like you playin’ Russian Roulette when you’re smokin’,” one man told researchers — but that risk gets overlooked when addiction persists.
The DEA reports that the potential lethal dosage of fentanyl pills has decreased from eight out of 10 being fatal to only three out of 10, but that has resulted in users taking more pills to feel the same effects or resorting to powder, which is harder to precisely dose.
“The opioid dependent community is ingesting more pills, knowing that the potency has gone down and that the recipes have changed a little bit on the Sinaloa side of the manufacturing,” Oz said. “If you’re taking more, if you get one hot pill in your mix, that could likely cause an overdose.”
But Oz is more concerned about carfentanil, a synthetic opioid that the DEA says is 100 times more dangerous than fentanyl itself.
Last March, the DEA saw an influx of carfentanil in the Arizona market, which Oz called an “anomaly.” In May, the agency put out a nationwide alert warning about the surge of carfentanil, which is so potent that it’s known to require more than one dosage of naloxone to reverse an overdose.
“Fentanyl scares me,” Oz said. “Carfentanil keeps me up at night.”
[emphasis added]
There are no surprises here. The behaviors described have always been known for highly dependent, high-risk opioid and other substance users – intently focused, determined, successful efforts to seek, find, and use closest substitutes and alternatives to the “drug of choice”, the substance that has been providing the desperately needed temporary relief from inner distress, fear of distress, and fear of facing the psychic/emotional roots of distress.
We saw it in Baltimore, where opportunistic use of risky, unknown, purportedly opioid samples led to a mass overdose event, followed 8 days later by a similar instance of desperately indiscriminate use of an unreliable supply, and repeated for a third time within 3 months.
[back to our current post]
And from another recent post, in Montana –

According to the Montana Department of Health and Human Services, the number of drug samples testing positive for fentanyl was cut in half between 2024 and 2025.
A decrease that large likely means there is less fentanyl on Montana’s streets. But that didn’t equate to fewer overdoses.
Ambulance services responded to roughly 250 more suspected opioid overdoses in 2025. That’s a 35% increase compared to the previous year. Overdose deaths also ticked up slightly.
The same picture for Columbus, Ohio emerged from this reporting, in late 2024, of persistent, worsening high-risk fentanyl use in an unpredictable drug supply, users depending on increasing provision to them and reversals by naloxone to be revived – to seek out and use fentanyl, again and again. As described in this post –
COLUMBUS, Ohio – The death toll from fentanyl and other synthetic opioids is falling for the first time since the drugs began flooding America’s streets a decade ago. Users and police in this city’s beaten-down Hilltop neighborhood credit another drug flooding the United States: the overdose antidote naloxone.
James “Sleaze” Morgan says naloxone has saved him after overdosing – as many as 20 times in the last several years.
The lifesaving nasal-spray medicine is everywhere in the 10 or more Hilltop “trap” houses where users come to buy and take fentanyl. Distributed free by local officials, supplies are abundant at the house where Sleaze smokes fentanyl and works security in exchange for drugs.
[emphasis added]
…
But the stories of Sleaze and other users in Columbus show how even with a powerful antidote on the streets, it’s proving difficult to break fentanyl’s grip on America.
[emphasis added]
…
Scott Sanders is executive director of the Hope Resource Center, a haven and support provider for Sleaze and other users in the Hilltop area of Columbus. He hands out roughly 1,000 naloxone kits a month, each with two nasal-spray canisters. But while naloxone is saving lives, Sanders says, the number of substance abusers on Hilltop’s streets is growing.
Visits to Hope’s drop-in center have risen about a third this year, to about 18,300 in the 12 months through November 2024, up from about 13,400 in the prior 12 months.
“And that scares me to death,” Sanders says. “Because all the powers that be are going to be throwing parties. Like, wow, look, it’s not a problem anymore,” he says of the fatality trendline. “But we’re busier than ever.
[emphasis added]
Back to our current post.
It’s the same situation in Ontario, Canada, where increasing high-risk use in street economies of unpredictable illicit drug supply has opioid overdoses surging, yet successful naloxone campaigns are reducing or moderating fatal overdoses.
It is, in fact, the same everywhere.
Reality check and reminder: for expert gold standard treatments, fentanyl test strips, illicit drug interdiction, or any form of supply variation to possibly be credited with a role in reducing opioid deaths, their implementation must reduce high-risk opioid use and overdose. Must.
In contrast, if high-risk use and opioid overdose are increasing, while opioid fatal overdose rates are moderated or reduced, that can only mean one thing – that naloxone campaigns are the cause of reduced deaths.
Although that question is answered for our example of Allegheny County, PA, the picture clear from available reports, we fortunately also have direct evidence, and that evidence happens to rule out all factors other than naloxone.
The figures come from the Allegheny County Overdose Dashboard.
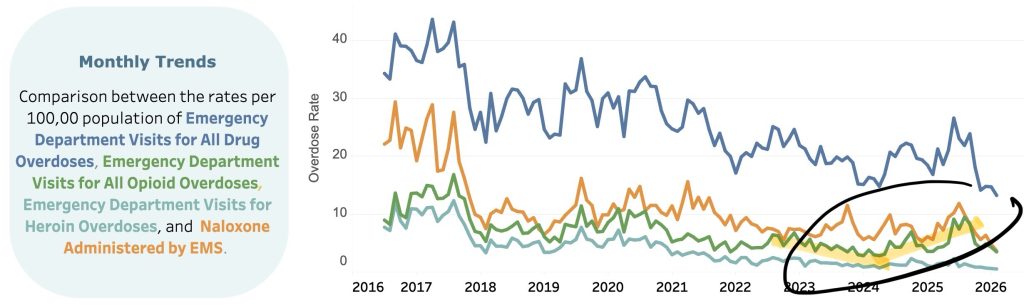
Emergency department (ED) visits for all opioids, a valid measure of high-risk use and overdose trends, quite clearly shifted from a decreasing trend to increasing leading into 2024 and 2025.
That’s congruent with the data represented as annual rates.
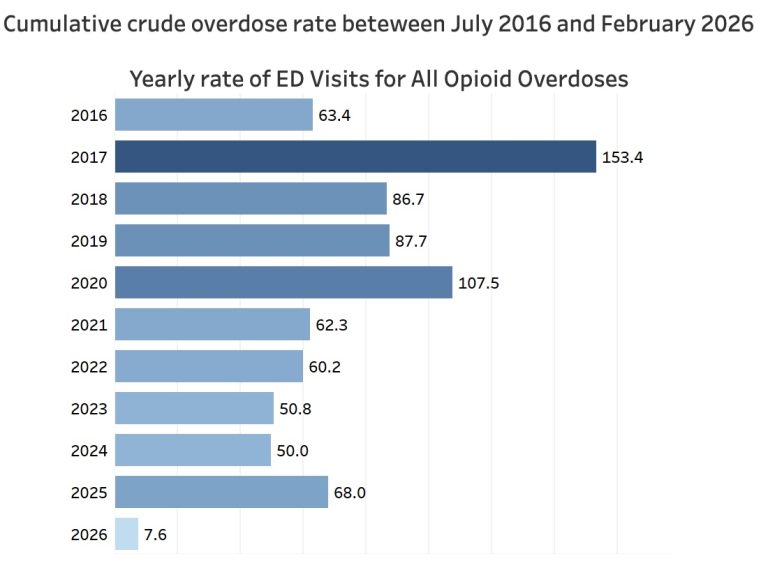
A three-year decreasing trend ended in 2024, and the figure for 2025 is the greatest since 2021.
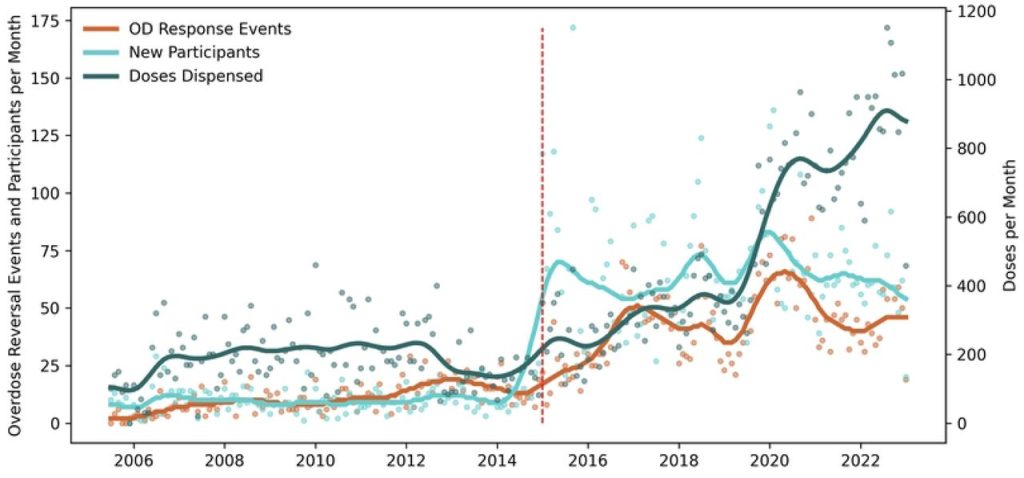
Supply changes, treatments, other factors are ruled out as explanations for dramatic drops in deaths in 2024 and 2025, when high-risk use and overdoses were increasing, and it is not a freakish coincidence that naloxone distribution in the county begain to surge in the years running up to those drops.
Statewide in Pennsylvania, as described in this post, funding, coordination, and community-based distribution of naloxone surged dramatically in 2023, just ahead of the drops in OD deaths.
In this May 2025 news piece, Pittsburgh officials involved in funding for opioid crisis response attributed the OD death drops beginning in 2024 to those efforts.
There is not a way to paint a different picture here,
no matter how reassuring or comforting it would be to be able to believe that the vacuum of thought represented by the expert and media assertions and conveyances, the demonstrated absence of capacity to form cogent thoughts about a lethal, worsening public health crisis, somehow are an exception in this specific example, for the questions about trends and factors we have considered.
But that’s not possible, because the intellectual cowardice and diminished capacities have run through the entire course of the opioid crisis, from the beginning, from all appearances as characterological traits and features tied to the ascension of those endowed to membership in America’s expert and media classes.
That true picture, provided over the past six years in hundreds of posts here, is the only way to understand how lethal absurdities as ungrounded and demonstrably invalid as the very conception of “addiction” let alone as a disease of the brain, or of medicalization of chronic pain, compulsive substance use, or depression, could possibly have arisen, become established, become doxa.
“Crisis is a necessary condition for a questioning of doxa, but is not in itself a sufficient condition for the production of a critical discourse.”
– Pierre Bourdieu Outline of a Theory of Practice (1972)
In Bourdieu’s Theory of Practice, heterodoxy is dissent, challenge to what “goes without saying” – the accepted, constructed doxa, “knowledge”, reality, that goes without saying precisely because it “comes without saying”, without real scrutiny, untested, unquestioned. The function of doxa is not knowledge or truth or promotion of the collective good, but to protect and serve the interests of those with the power, the cultural capital, to create it.
Egregious examples include the profoundly impaired capacity of top researchers to understand the failed outcomes of their $344 million megastudy confirming the lethality of “gold standard” medical treatment, let alone understand the imposed interpretation of outcomes required by their own research design, the clueless distortions helpfully hidden by equally impaired reporting in major media.
More recent examples, from last week’s post, include harm-predicting public health misinformation generated by gross incapacity for critical thought, by wannabe expert mouthpieces for a new war on drugs, elevated as authoritative sources in major media.

The predictable failures and public harm are pervasive and persistent; those incapable or fearfully avoidant of critical thought, of truth seeking and telling, rewarded with protection by the systems of power that their useful errors and thought-free assertions keep intact, in power.
Their work and its impacts are everywhere, more and more effectively unified and messaged, seemingly intractable and unassailable.
Seemingly.
Yet all it took for us to dismantle and nullify the deceptions, to protect the truth, was a questioning, some research, and a desire to think freely and clearly.






