OPIOID CRISIS GOLD STANDARD CURE BUPRENORPHINE GAME-CHANGING SUBLOCADE FORMULATION: 30-DAY EXTENDED-RELEASE INJECTION A PREDICTABLE FAILURE
What could possibly go wrong with a new expert, doctor-approved formulation of opioid proven cure buprenorphine that can’t be diverted, abused, or stopped from working once injected?
by Clark Miller
Published August 8, 2025
It seems impossible to not feel the excitement and triumph messaged in media accounts of the dawning of the newest game-changing medical cure to vanquish a decades-long worsening opioid crisis.
Little research has emerged to date due largely to the expense of the once-monthly injections and to the resistance of high-risk opioid users to start the formulation despite apparent advantages, along with very low treatment retention including cessation and move back to other buprenorphine formulations, to methadone, or other medically dispensed substitute opioid – as we’ll see.
And we’ll see that these are important claims of benefit for which the answers we need are provided by evidence we have, not dependent on statistically analyzed research.
Here’s some of that excitement and confidence about injectable buprenorphine, “Sublocade”, from doctors and experts in California where its use in clinics had begun by 2022.
For a doctor providing Sublocade at an Oakland hospital, it’s a “game changer”, possibly his “only chance to help a vulnerable patient at risk of overdose”. That’s because, as explained –
Buprenorphine, one of three medications approved in the U.S. to treat opioid use disorder, works by binding to opioid receptors in the brain and reducing cravings and withdrawal symptoms. And because it occupies those receptor sites, buprenorphine keeps other opioids from binding and ensures that if a patient takes a high dose of a drug like heroin or fentanyl, they are less likely to overdose. Patients often stay on buprenorphine for years.
Not only is Sublocade a game-changer, but is “easier” to provide, and as explained by a doctor in Bakersfield, California, it simply eliminates any compulsion to use a high-risk opioid user might otherwise have, because due to the Medical Science – “your cravings are gone, cravings are controlled”.

BAKERSFIELD, Calif. (KERO) — One of the newest methods of treating opioid-use disorder has doctors raving. It’s called Sublocade, a brandname extended-release injection of buprenorphine.
“It’s incredibly effective,” said Dr. Matthew Beare, medical director of special populations for Clinica Sierra Vista. “The purpose of it is is to get rid of those opioid cravings but at the same time offer some protection.” ..
“Imagine fentanyl binding to opioid receptors and dialing them all the way up to an 11, potentially causing an overdose. Well Suboxone, buprenorphine, and Sublocade bind to the exact same receptors, but they only activate them to about 40 or 50% of that,” Beare said. “What that means is because you’re getting some activation of the receptor your cravings are gone, cravings are controlled. Because the activation isn’t dialed up as high as the other one, it’s very hard to overdose on it.”
If that’s not clear enough, here’s an explanation from a Michigan Sublocade doctor on how the injectable bupreneorphine can treat patients’ opioid addiction, “a type of substance use disorder that is classified as a neurobiological disease”.
What is Sublocade used for?
Sublocade is used to treat opioid addiction, a type of substance use disorder that is classified as a neurobiological disease. Addiction has genetic, psychosocial, and environmental factors influencing its development and manifestations.
A great way to think of how opioids and the medication works is to imagine your brain has a bunch of empty ice cream cones on it- we’ll call these ‘receptors.’ When the ice cream- we’ll call these ‘opioids,’ enters the space by the brain, they normally fit right into the empty cone. Unless you have a dairy allergy or are lactose intolerant, this will feel really good for most people.

This same mechanism is what happens for opioids (pills, drugs) in the brain, when they result in a release of Dopamine creating a sense of pleasure and reward.
Sublocade and the medication in it, buprenorphine, attaches to those ice cream cones making other scoops of ice cream less likely to park.
So, it does make sense that this new expert game-changing medical cure is about to turn the opioid crisis around!
In North Dakota, provision of Sublocade to incarcerated individuals is already being pitched for expansion, by Dr. Stephanie Gravning, health authority for the Department of Corrections and Rehabilitation (DOCR), to counties for use in jails.
“We began this in prison because there’s dozens of studies that show this can reduce illicit opioid use after people are released. It reduces criminal behavior post incarceration. It reduces mortality. It reduces overdose risk,” Gravning said. She also cited a Rhode Island Department of Corrections study showing that starting treatment while incarcerated significantly increased ongoing compliance after release, compared to starting treatment at release.
Her program has what may seem to an advantage, because the “DOCR can obtain a mandate through the court requiring a prisoner undergo treatment. DOCR’s preferred medication, Sublocade, is administered by injection once every 28 days”.
That Rhode Island DOC study she alluded to is most likely the one described here.
In Maine, Sublocade in jails is more than a game changer, it’s “revolutionizing addiction treatment“.
Since beginning in 2022, more than 200 inmates have been provided the new formulation.
Dr. Alane O’Connor is the medical director for Maine Maternal Opioid Misuse Program, or MaineMOM, as well as Perinatal Addiction Medicine at Maine Medical Center. She started the program at the jail in July 2022 with the partnership of Somerset County Sheriff Dale Lancaster; jail administrator Capt. Michael Pike; programs manager Michael Welch; and others clinical staff.
“I want to keep people alive, and the hope that this gives patients is remarkable,” O’Connor said. “I think that it’s been super clear for a long time that the patients that are highest risk are the folks that are coming out of jails. The opportunity to make significant changes is really in a correctional facility.” …
Ellis [Greg Ellis, Physician Assistant (PA)] celebrated the fact that the injection option effectively eliminates the diversion potential.
“It can’t be diverted. And, more importantly, it gives a steady state of release,” Ellis said. “They can’t choose not to use it. If somebody in a Suboxone program has a bad week, breaks up with their girlfriend again, in a risky moment says, ‘Forget the Suboxone; I’m going to go to heroin today,’ they can’t make that choice. By having the Sublocade on board because of the affinity or its strong attraction to the receptors, it’s protective in some way.”
[emphsis added]
That truly would be remarkable, that someone with the injection “can’t make that choice” to abuse other substances while using Sublocade.
We’ll get back to that.
In Missouri, doctors are excited about the game-changer too, have been beginning as early as 2018, a year after FDA approval.
It’s been provided in the St. Louis county jail beginning November 2024.
Dr. Mikel Thomas of Phoenix Medical Research, has tested hundreds of drugs in the battle against opioid addiction.
“We have never seen people’s lives change like this has changed lives,” Thomas said. “There’s a freedom to (Sublocade) that we did not have in other trials we’ve seen. ..
Often, patients like Palmer try to get clean with traditional Suboxone pills, but with the new drug, people using the shot can’t get high if they try to take drugs on top of their medication.
[emphasis added]
They “can’t get high”; no wonder experts are assuring us and media conveying that we’re headed toward the end of the opioid crisis.
In Chicago, Project LIFE (Long-acting Injectable for Ending Overdose) has been administering Sublocade beginning 2023 or earlier.

In Seattle, Washington, a behavioral health treatment provider, Downtown Emergency Service Center, began providing Sublocade to high-risk opioid users last year.
The potential breakthrough comes as fentanyl continues to kill hundreds of people in King County each year, many who are homeless, and as elected officials turn to arrests to crack down on people who use it in public. ..
“It could totally be a game changer,” said Nathan Kittle, addiction medicine specialty director at HealthPoint, a nonprofit community health center in King County. …
Emmalee Laing and John Slack, a couple who began receiving buprenorphine injections through the new protocol about six months ago, say their fentanyl use is about a quarter of what it used to be.
“It’s become more social than actually like physical dependence on it,” Slack said.
Laing started delivering takeout for Uber Eats using a scooter, which is a big deal, she said, since it’s the first time she’s cared about getting a job.
Each month she receives an injection, her cravings have become weaker.
Both she and Slack, she said, want to stop using altogether.
“I feel like both of us are actually close to that.”
Uhhh … okay … wait …. WHAT?
Six months on the newest game-changing medical opioid cure, and they’ve gone from using illicit fentanyl maybe daily or most days to … 6 or 7 days in a month? That sounds more like “bridging”, around for a long time, actually facilitating and enabling high-risk heroin or fentanyl use with medically dispensed buprenorphine to take a tolerated break between getting high with real dope again.
With the current risks of street fentanyl use, what does “social” use look like? What could drive taking that risk?
Is the diminution of cravings provided by six months of treatment with the new medical gold standard not quite enough to deter risking fatal overdose 5 or 6 or 7 times each month?
That would be a great question for the Sublocade patient in Alaska, where Sublocade has been in use for a while.
Spencer and Hubbard said they’ve seen many lives transformed by buprenorphine.
D said getting on the long-term injection has been the best thing for him.
“Sometimes I still get high, but it’s way less often, like maybe once a month or twice a month compared to every day,” D said. “When you’re addicted to heroin, you have to have it every day, otherwise it’s not going to be a good day. Believe that.” …
Addicted to heroin maybe, but it was fentanyl D used to get high and was positive for last time he ended up in jail while on the injectable “bupe”, Sublocade.
“I knew I had to go to jail, so I wanted to get my shot before I went, so I didn’t get sick when I went in there,” D recounted. (Alaska Public Media is identifying D only by his first initial because he’s worried about his safety.) ..
After Spencer gave him the dose of buprenorphine and he was arrested, he went to jail and tested positive for fentanyl, he said. He hadn’t used fentanyl in two weeks, he said, but the positive drug test meant he was denied further medication.
“I thought it wasn’t fair,” D said. “Relapse is a part of recovery.”
The picture for Sublocade seems to be shifting, doesn’t it?
The more information we consider about it, its use, and claims made for it?
Good thing there’s this news piece from Philadelphia, in which we gain some significant details about the Sublocade experience, its medical provision, and some clarity.

At Prevention Point Philadelphia, officials report that interest in long-acting medications for opioid use disorder is growing significantly. The organization administered 312 Sublocade injections in fiscal year 2023 and double the number in fiscal year 2024.

Sublocade got approval from the U.S. Food and Drug Administration in 2017. While it’s been around for several years, Prevention Point clinic Dr. Serge-Emile Simpson said there have been challenges to prescribing it in the past.
It has a higher price tag compared to some other medications for opioid use disorder, so getting insurance to cover it was a problem. There was also special training required for providers who wished to administer the drug, Simpson said, and maintaining a local supply of the drug often came with other delays.
Now, more insurance plans cover Sublocade, and Prevention Point has a standing order with a local pharmacy to make sure the medication is readily available.
But there was still another hurdle to overcome, Simpson said. Providers noticed that some people in Kensington sell portions of their Suboxone prescriptions, a daily oral buprenorphine medication that comes in dissolvable strips, out on the street.
The people selling the medication would then use the money to buy food, clothes, bus tickets or even street drugs, while people buying the Suboxone would use it to manage withdrawal symptoms between injections or hits, or to supplement their own Suboxone treatment if they felt like their dosing wasn’t high enough to feel well, Simpson said.
“We could not get people interested in Sublocade because it would have bitten into their cash flow if they were selling some or all of their Suboxone,” he said. “That’s a significant sort of impediment to getting them started.”
That’s one way of describing the situation. Here’s another, from a previous post, outlining the central roles – as commodity, consumable, currency, other roles – buprenorphine has played in facilitating and fueling illicit economies of street opioid and other high-risk drug use.
From that previous post –
“Who needs Suboxone? I got Suboxone,” said another man, who was apparently trying to sell the brand name medication for addiction treatment.
That’s from an “on the street” report from wbur reporter Deborah Becker late October of last year, about 4 months ago, from the “Mass. and Cass” area of homeless encampments and methadone clinics in Boston.
It is illustrative of the inconvenient and downplayed phenomenon known and established for decades for every American city, for every area in the U.S. where there is illicit drug use and trade.
American Medicine’s gold standard “addiction treatment medication” Suboxone (“subs”, “bupe”) is one of the most widely diverted, available, in demand, used and abused, traded and bought or sold drugs in America’s illicit street and prison economies of illicit opioid and other drug use. That’s been known and established for decades, described additionally here and here (scroll down to “The bupe economy”).

If you’re familiar with these areas of the role of Suboxone as consumable, commodity, and currency, including for fentanyl, in lethal economies of illicit drug use, scroll down to the next section, headed, “Back to our current post”.
The important and fundamental point is that for decades, from the beginning, “bupe” has been in those economies, pervasive, easily obtained, and cheap, as partly described in a recent post.
Here, for example, is another on the street description of the longstanding bupe economy from a few years ago.
“Subs. Who needs subs?” a woman called out quietly near the intersection of Kensington and Allegheny avenues on a recent afternoon. She had to be careful. This district, on the northern fringe of the city’s so-called “Badlands,” is clustered with loosely organized crews hawking pharmaceuticals from Percocet to Adderall. Drawing attention could get her banned from the corner, or possibly worse.
Like many people who are dependent on opioids in Philadelphia, the woman was freelancing—likely selling off the last of her own prescription for the popular opioid substitution medication for money to purchase heroin/fentanyl. It’s something I’ve seen countless others do during my time covering the overdose crisis.
A passer-by inquired how much. “Five dollars,” came the reply. The man kept walking. “Wait, wait,” the woman said. “Give me three.”
And with that, the man acquired his Suboxone at less than half the retail price of a customer paying in cash at their local pharmacy. . . .
Meanwhile, diverted “subs,” as they are still universally known on the street, are all over Kensington, where the sublingual orange-flavored strips typically sell for $10 a piece, equal to the cash price of the drug at pharmacy chains like CVS or RiteAid. (The pills, which are less desirable because they’re harder to split and reportedly make the mouth water, generally sell for half the price of a strip on the illicit market).
Subs are now the most commonly sold pharmaceutical here. And unlike Xanax or Percocet, which are often counterfeit pressed pills that sometimes contain fentanyl, all of the subs on the streets are diverted from legal channels. . . . Several street-level sources have told me that subs’ illicit availability has made “chipping” (using heroin only occasionally and filling in with burprenorphine) possible for them for the first time. Others carry a strip or two with them to ease the symptoms of withdrawal in jail (or turn a quick profit for the commissary) in the event they are arrested. A single 8 mg strip of Suboxone costs as much as $80 in county jail, and is typically cut into tiny pieces to maximize return. . . .
One thing seems certain though, given the sheer abundance of the drug on the street: Many people who have a prescription for Suboxone, who may get it free through county medical assistance or at a reduced cost through the Obamacare exchange, are not taking it.
Back to our current post –
So, for high-risk opioid users continuing to use, free buprenorphine has high value on the street.
Unless it’s Sublocade, injected under their skin.
At Prevention P0int in Philadelphia, they came to a solution, of sorts –
Prevention Point added an incentive program to its Sublocade treatment, where patients get $100 in gift cards for their initial monthly shot and then $25 every time they come back to continue their monthly treatment.
Simpson said while it may seem controversial, the model has been successful in keeping people in treatment and recovery, reducing their use of street drugs and supporting them with a way to buy food and other daily items.
“reducing their use of street drugs”
“supporting them with a way to buy food and other daily items”
Evidence for that? None available for the news piece?
Here’s some evidence from a recent Canadian study of Sublocade.
Highlights
Extended-release injectable buprenorphine (XR-BUP) may address some adherence challenges.
Real-world evaluations of XR-BUP outside the U.S. and high-risk populations are limited.
Cohort study of 25 adults with OUD and high risk of overdose starting XR-BUP in Canada.
XR-BUP was well tolerated.
Six-month retention rates were low and most continued to use illicit opioids.
[emphasis added]
Let’s recap
Medical provision of the new, promising, game-changing medical opioid cure, Sublocade, has been to varying degrees initiated in a variety of states and locales reviewed in this post:
California
Missouri
Philadelphia
Maine
North Dakota
Seattle, Washington
Chicago
and Alaska
Considering recent trends in changes in opioid overdose deaths among states, none of those locations stand out as having notably benefitted compared to the national range and distribution. If Sublocade had been working as assured by experts, they should as a group be near the top among states.

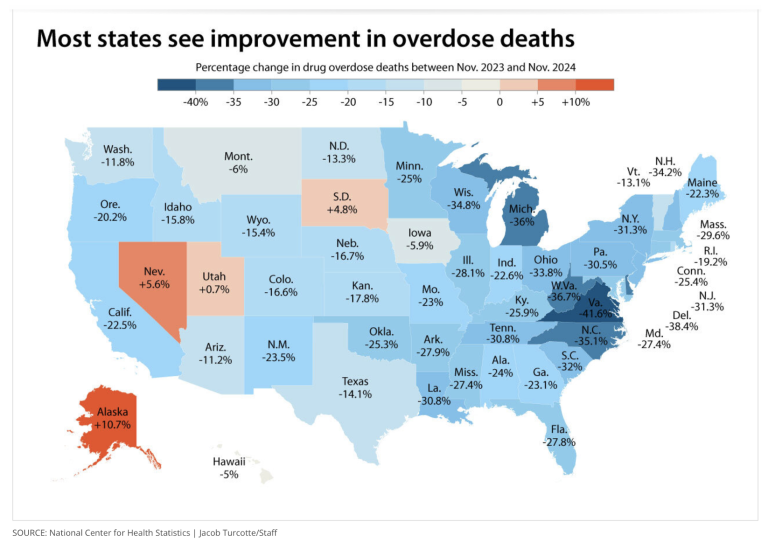
In programs in Seattle and Alaska, by direct report enrollees continued to engage in regular high-risk use of opioids (fentanyl), a result consistent with research from Canada where 72 percent of Sublocade patients continued to use illicit opioids.
Related evidence establishes that any and all recent drops in opioid related deaths have been entirely attributable to naloxone campaigns in Sublocade locales: Philadelphia, in Seattle, and in Chicago.
In Philadelphia, surveyed community members see a worsening crisis, very few (8 percent) see improvement.
In the end, all of those considerations are peripheral to what underlies these results: for almost all high-risk opioid users, the Sublocade formulation has no value to them. It cannot serve as currency for fentanyl like other forms of buprenorphine, nor like them can it be used intermittently to “chip” or “bridge” to avoid being “dopesick” between runs of illicit opioid, “real dope” use, nor sold for cash to someone feeding the prison bupe economy.
Those are the reasons recruitment in these programs has been so challenging, the reasons in Philadelphia why opioid users have to be paid to take the Sublocade, paid to take the game-changing medical cure that stops cravings and saves their lives.
More fundamentally for any opioid user wanting to stop use, like all agonist or partial agonist opioids, it has no treatment value. The forces driving persistent compulsive opioid use have never been about physical “cravings”, always about deep psychological distress, about psychological pain, fear, and the learned helplessness instilled in users by pathological systems of care that are their only known options.
Sublocade, the best medical cure formulation experts have to offer, is no game-changer.
It is predictably the new Suboxone, every bit as useless, every bit as lethal, and more profitable.






