ROUNDUP OPIOID CRISIS: PREDICTABLE FENTANYL TEST STRIP FAILURE; HARMS/BENEFITS OF CRISIS-CAUSED PUBLIC HEALTH DISRUPTIONS; SACKLER FAMILY BURNED AT THE STAKE
Nothing is what they desperately need you to know it is.
by Clark Miller
Published May 15, 2026
The opioid crisis ‘harm reduction” measure of provision of fentanyl test strips (FTS) just appeared in the news again, this time interestingly as a political broadside by The Guardian disguised as an “Analysis” with important information conveyed by an American expert on the topic.
The piece starts like this –
Within just a few weeks, the Trump administration has proposed multiple contradictory policies related to overdose prevention – some that could help save lives and others that experts say could further strain health resources and put people at risk for overdose.
These policies include a new prohibition on funding for fentanyl test strips, which help people avoid overdoses; proposed budget cuts that would gut the country’s overdose prevention efforts; and an ambitious drug control strategy that will be impossible to implement if the aforementioned cuts go through.

So, we know that use of FTS saves lives, it says so right there in the second paragraph of the Analysis, about the ” … fentanyl test strips, which help people avoid overdoses”.
So, that’s a fact, not even requiring a link to a different article or research paper providing evidence for that benefit, that’s how well established that is. It “goes without saying”.
At the very least, we can be certain that distribution and use of the strips does not predict harm or increased risk.
And yet, these very issues are generating political attacks and ammunition, and worse, are “confusing experts“, which may affect our levels of trust in their expertise.
Additional designated experts sounded warnings even more dire and dramatic in the Guardian’s follow-up piece two days later, that –

It seems we are compelled to take a look
and to think about what is being conveyed by our expert/media class.
One renowned expert who has no doubt that FTS save lives is featured in the Guardian piece, Dr. Nasbarun Dasgupta, director of the University of North Carolina’s Opioid Data Lab.
Readers here, and here, are familiar with Dr. Dasgupta’s understanding and with reliance by media upon it for insights and expert guidance on the opioid crisis, familiar from multiple posts including here and here and here.
From the Guardian’s Analysis –
An April letter from the Substance Abuse and Mental Health Services Administration (SAMHSA) indicated the agency would no longer fund test strips for fentanyl and other dangerous adulterants that are “intended for use by people using drugs”. Dr. Nabarun Dasgupta, director of the University of North Carolina’s Opioid Data Lab, said defunding test strips “is a win for the cartels”, noting that it will take away people’s ability to identify impure products and flag it to their dealers.
[emphasis added]
Huh! Okay, let’s think about that, to attempt to discern the mechanism, the realistic social and illicit drug economy interactions that would be required, necessary, to expect that type of outcome that starts with a high-risk drug user obtaining a positive result for fentanyl in drugs obtained for use, then somehow that information making its way to some level of dealers or suppliers at which changes would result in a safer drug supply free of fentanyl or other, even more potent synthetic opioid creating the risk of fatal overdose.
Now, how does that work?
But first some important background information.
1.
The test strips (FTS) provide only a result of absence from or presence in a drug sample, do not provide information on the quantity or potency of fentanyl (or other HPSOs = high potency synthetic opioids) in a sample.
2.
Most fentanyl users are seeking fentanyl, so why would they test? They probably wouldn’t, although a negative result in drugs bought as fentanyl would be valuable information, but not to deter the high-risk user, headed toward onset of withdrawal symptoms, from seeking fentanyl and not with other protections against high-risk use and overdose.
3.
The common use and potential for information gained by high-risk users comes when drug samples of other preferred substances are tested, like meth, cocaine, illicit benzodiazepines, and other drugs, all complicated by the potential for contamination by fentanyl and other HPSOs in current street economies of illicit drug use, as partially explained here, for example, and here, and here.
It gets complicated, because in addition to high-risk users who want to reduce the risk of overdose from the cocaine or meth they’re getting, others are seeking fentanyl as an addition to those stimulants, due to the desired, combined effects.
4.
In those street economies of illicit drug use, with use of fentanyl test strips, there is no safe use.
Even kids buying illicit vapes for THC or nicotine are at some risk of exposure to fentanyl and other toxic, added drugs.
There is no safe use primarily because, despite some test strips also detecting additional fentanyl-like substances, more of the rapidly evolving street presence of potentially fatal HPSOs are not detected.
Excerpts from an AI-generated summary:
- Acetylfentanyl
- Butyrylfentanyl
- Carfentanil
- Furanylfentanyl
- Sufentanil
Because new synthetic analogues are constantly being developed, the detection capabilities of these strips may change, and they may not recognize every variation of the molecule. …
- The “Chocolate Chip Cookie” Effect: Fentanyl is often not distributed evenly throughout a sample. A small portion tested may be negative while another portion contains a lethal dose.
- No Indication of Potency: A positive result indicates the presence of a detectable amount, but it does not specify the concentration or the total amount of the drug present.
- False Negatives: A negative result is not a guarantee of safety. Many potent synthetic opioids, such as nitazenes or certain new fentanyl analogues, may not be detected by standard test strips. …
As of early 2026, fentanyl test strips (FTS) are effective at detecting fentanyl and many of its analogs, but they have significant limitations regarding new synthetic opioids, particularly nitazenes and “orphine” analogues. These newer synthetic drugs can be up to 40 times more potent than fentanyl and are frequently added to the illicit drug supply
[emphasis added]
5.
High-risk drug users using FTS are not doing so toward a goal of stopping their high-risk use; they are doing so to facilitate, to continue their high-risk use.
6.
Considering harm-reduction approaches, it is established that naloxone campaigns account entirely for all recent-year (and prior) decreases in fatal opioid overdoses across all U.S. states and locales.
The magnitude of year-by-year increases in deaths prevented by the intensive, desperate, successful naloxone campaigns more than accounts for all reductions in deaths. There are no reduced overdose deaths left to be attributed to other measures, like FTS or supply disruptions, effects of which are nullified by examination and consideration of the evidence.
So, there’s that.
The contrast between use of nalxone to reverse an otherwise fatal opioid overdose – directly observed and quantifiable – and use of FTS could not be more lethally stark.
There are no observed or verified instances of use of FTS ultimately leading to an avoidance of what otherwise would have been an opioid-related death.
So, there’s that too.
But let’s try to imagine what must have been envisioned
by the expert Dr. Dasgupta to generate the claims about FTS.
Let’s imagine a high-risk user, with a finding of the presence of fentanyl in the methamphetamine obtained, in an encounter with the “dealer” he wants to “flag it to”, an encounter allowed by continued availability of FTS, and without that availability, “a win for the cartels” per Dr. Dasgupta.
User: Hey, I got a positive for fettie in that meth from Monday, no way I’m gonna take that chance.
Dealer: Oh man, hey, I usually test too, I dunnoh what happened. I apologize sincerely and I’m gonna take this up the chain, let my source know, so they’ll do something about that. You know, right? A lot of guys are looking for some fettie in that. I got no word of anybody with an OD …
User: Yeah, but …
Dealer: Okay, I know, I know. Know what, I’m gonna dump that whole bag, flush it. No sense takin a chance. I’ll get pure next time, even if it costs more. And my source is gonna let his man know. It’ll get straightened out! So, you hold Narcan too, right? And use with somebody? That’s how everybody copes.
Hey, meanwhile you need something right? I got some pills, can I hook you up?
That user would now be satisfied that the right people will get the message, that thanks to fentanyl test strips, “people’s ability to identify impure products and flag it to their dealers” will ensure the safety of their source of meth. He may not even feel the need to test again?
Right?
But we don’t need to rely on imagining or speculation, because there are clear, powerful ways to evaluate the proposed fiction by use of evidence.
It’s simple, really,
as with naloxone and naloxone campaigns, the course of legal, policy, and institutional support for use and distribution of FTS has varied widely across states and locales in the U.S.
Early FTS adopters in 2017 to 2018 included San Francisco, Philadelphia, North Carolina, New Jersey, and New York City. As of 2022, only about half of the states had made possession of FTS legal; now most have.
A powerful evaluation, of course, as we have done here for naloxone as harm reduction, would be to look at a variety of differences and gradients in locale and time to compare the development of FTS provision, support and use across differences to patterns in the conjectured outcome of less toxic (contaminated, dangerous) drug supply due to high-risk users asserting complaints about their positive FTS results.
We are all compelled to do that, to research that, in order to avoid the real, grave error of attributing protective benefit to FTS if there is not. And to prevent harm and deaths by overdose if, for example, false security in the belief that a negative FTS result leads to continued high-risk use with drugs that may well be lethal, the result supported by a published research report last year. We’ll get to that soon.
We are compelled to consider, for example, whether in San Francisco, with the longest history of support for FTS, the street drug supply is any less toxic, any less dangerous due to potentially fatal adulterants than in other locales.
And compelled to consider the rise in high-risk use and overdose in Montana, where FTS has been supported since 2021, where detection of fentanyl in street drugs recently decreased, and where “the drug supply is more complex than it’s ever been and remains dangerous“.
From that report –
Adams Sibley is with the University of North Carolina Chapel Hill’s opioid data lab. It tests illicit drugs from all over the country.
“I would say that we’ve moved from a crisis mostly driven by fentanyl, to a crisis driven by adulterated fentanyl, specifically with sedatives like xylazine and medetomidine,” he says.
And compelled to consider the situation in Arizona, where FTS has been supported since 2021, and an increasingly unstable, dangerous street drug supply is associated with increasing high-risk use and overdose.
And? We have a research report,
published May of last year.
We’ll stick to the salient outcomes and points. In this study, two groups of high-risk drug users from different locales where FTS was available were compared. One group had been using FTS, the other group had not.
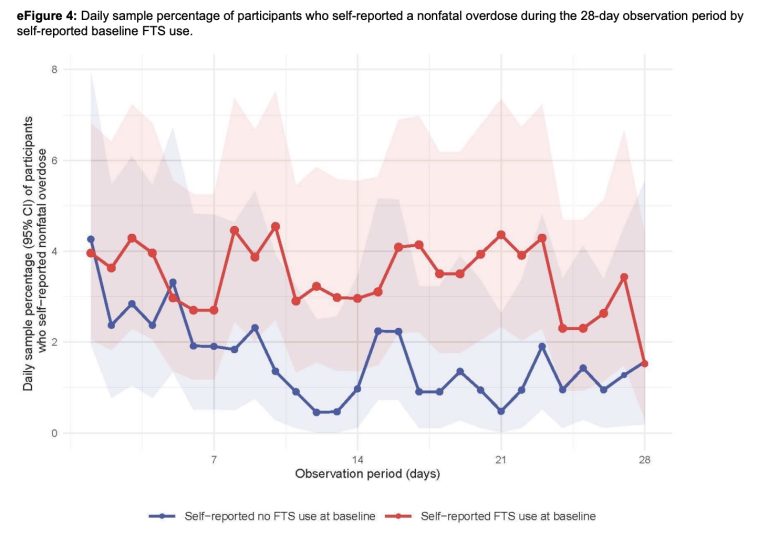
Over a period of surveys of them, FTS users reported slight differences in the number of different additional harm-reduction measures they engaged in (e.g., using a smaller amount of a drug, “throw out drugs because they were bad or not what you expected”) and how often they engaged in those safety behaviors, compared to the group who had not been using FTS.
Except for the single most important, critically important, of those outcome measures – whether, when they did use a drug, “Someone else was present when you used drugs”, the life-or-death factor in the case of an overdose, when seconds count and proximity of someone with Narcan is critical. There was no greater engagement in that protective factor for the FTS-using group.
More to the point, there was no difference between the two groups in the only outcome measure that really matters – the reported number of overdoses. The number of overdoses was no fewer, not different, for the FTS-using group. With a statistical test P value of .52, the outcomes were way not different. That was for the adjusted risk ratio comparison, a statistical method to improve power and validity of a test by adjusting for covariations between groups in factors like demographic differences, drug use differences, and others. For the non-adjusted risk ratios, reported overdoses were actually higher for the group using FTS.
Let’s move on.
An apparently very popular and very effectively promoted photo essay appeared recently, describing anecdotally observed and collected personal impacts on problem substance users affected by Hurricane Helene.
It was picked up by numerous outlets and was prominent in “opioid crisis” online searches for days in a row.
The writer, a public radio climate change reporter, did not hesitate to generate and assert powerful conclusions about the nature of problem substance use, the needs for successful change for those experiencing compulsive substance use, and the therapeutic value of social and other factors, beginning with the designation of known, established
“systems that keep people sober“
and with this, in the subhead,
“Recovery from substance use disorder requires community”
That appears to be a very touching, resilient, and beloved sentiment generally in media accounts.
Does it capture truths? Or predict harm?
The opening paragraphs answer those questions for us, with prose as maudlin, distorting, deceptive by omission, and harm-predicting as it is appealing and soothing, no doubt, for many readers. What could be more heart-warming and sympathy-intoxicating then an American war veteran, a 5-year-old daughter, and the image of penitent, grateful others gathered and joined in spiritual unity to identify as “addicts”, expose their defects, and accept the saving grace of their Higher Power?
As Hurricane Helene roared through the mountains of western North Carolina in September 2024, Devon ran from one side of his house to the other, listening to the sound of trees snapping in the dark.
The wind whipped the steep hill his family lived on in Asheville, rattling the windows and cracking limbs. Pine trees fell like dominos, 20 in all. Five of them took the porch and a corner of the house with them. The creek behind the family’s home was rising fast, and anything caught in it was swept away.
Inside, Devon’s wife and their daughter, who is now five, hid in a closet, crying as the house shook. Devon shouted over the wind as he tried to figure out what would fall next. He was inside the house, but also somewhere very far away, reliving memories he had been trying to put away.
“For me, it was very triggering,” he said. “I felt like I was in a war situation.”
Devon, an Iraq war veteran who moved to the mountains from Florida in 2019, asked to be identified by only his first name, as anonymity is a core component of 12-step programs. The 41-year-old had returned from the Middle East in 2006 with post-traumatic stress disorder and a traumatic brain injury that pushed him to numb himself however he could. It started with pills, then heroin, and eventually a combination of heroin and cocaine. “I was so physically addicted,” he said. “The sickness was unbearable. I couldn’t imagine life without drugs.”
In Asheville, he slowly found his way back from the precipice. He joined Narcotics Anonymous, attended regular meetings, and began to confront his trauma in therapy. He and his wife, who had moved to Asheville with him, had a daughter in 2020. It wasn’t always easy, but life with his family, in their house in the woods, felt like it was creeping toward stability.
Everything changed after the storm.
Disasters like Hurricane Helene level communities and upend even the stablest lives. For people recovering from addiction, they can also fracture so much more: 12-step meetings, treatment programs, transportation, and the social networks that are essential to maintaining sobriety. When that scaffolding breaks down, the risk of relapse and overdose rises.
We’ll come back to Devon, the falsely and dangerously constructed picture of his experience of NA, and what we know to be true about that religious subculture, it’s important.
But first, let’s consider the nature of the other few anecdotal accounts of experiences of hurricane survivors that are used to support the claims,
“Recovery from substance use disorder requires community” … “and the systems that keep people sober”
and what that could possibly mean.
One of those anecdotal accounts, prominent in the story, seems to require quite a stretch to conceptualize as necessary for persons in recovery, the area’s bars and nightclubs, locales that John Kennedy and his wife loved to frequent as a way to be socially connected, “Just the ability for people — like a church service, like a job — to show up and come in and be able to check on everyone, check in on everyone, see how people were doing,”
The bars and nightclubs, where he would drop off Narcan units, for customers and were “like a church service”, triggered great dismay when in the aftermath of the natural disaster, they were “shuttered, shuttered, shuttered”.
Any extra distribution of Narcan units is valuable, and yet is it a bit of a stretch – a bit bizarre actually – to provide this anecdote as supporting bars and nightclubs as one of the lost “systems that keep people sober“, especially in the context of North Carolina’s development of a robust, expanding, hugely successful system of Narcan disturbution beginning pre-pandemic and targeting individuals at highest risk?
There’s the story of Jeremy Haney, who “lost nearly everything: his apartment, most of his belongings, and Troublesome Creek Stringed Instrument Company, where he built mandolins by hand.” But not in Hurricane Helene, instead in the flooding in Kentucky in 2022, to make a point. What point is unclear. He stayed where he was, even though “now I’m going to have to start all over again.”
But that was better for him, anything was better than returning to Morgan County, where he grew up, must have had family and friends, connections. Morgan County was hit less hard than other areas of Kentucky, serving as a resource provider for displaced persons from outside the county.
Jeremy was afraid of returning to high-risk drug use there. What must we conclude? That community can be your worst enemy? For Jeremy, Morgan County was. And, it wasn’t “community” that was required for Jeremy to put things back together, instead two state programs and the professionals administering the benefits that allowed him to stay and continue to escape his home “community”.
The desired, needed, soothing, idealized folklore of “community” as the saving force is a distortion, a fiction, hijacked in a story that ultimately provides a picture of such community services as beneficial and required for success of persons experiencing problem substance use.
The gist of the extended piece on natural disasters is that community-based local addiction treatment programs, medical opioid medication -based treatment, and engagement in meetings and prescriptions of the religious subcultures AA and NA, are not just beneficial, but necessary, to “keep people sober“.
The problem is that it’s all a lie, and an increasingly lethal one, as substance use epidemics worsen.
It’s like a heart-warming, touching, family-rated Disney movie produced to convey an entirely fictional view and promote the use of failed systems that predict harm.
A lie like a G-rated feel-good movie with a highly stylized screenplay written by, or exactly as if written by, individuals who really, really want to continue to be dispensed opioid drugs by medical providers, and who really, really like the idea of having the unassailable status of “working a spiritual program” in AA or NA, America’s designated recovery religious subculture.
Disasters like Hurricane Helene level communities and upend even the stablest lives. For people recovering from addiction, they can also fracture so much more: 12-step meetings, treatment programs, transportation, and the social networks that are essential to maintaining sobriety. When that scaffolding breaks down, the risk of relapse and overdose rises.
[emphasis added]
Social networks? The examples we’ve been provided in the article include escape from and aversion to home community social networks in Kentucky from fear of relapse and bars and nightclubs as therapeutic social networks in North Carolina.

What about 12-step meetings and treatment? We can be brief, because this is not complicated.
It turns out that American non-medical “treatment” for “substance use disorders” (SUD), that is, for compulsive behaviors constituting problem substance use, treatments described variously as “rehab”, “treatment” “SUD treatment”, or “addiction treatment”, is not treatment at all and does not provide benefit, described in multiple posts here, for example here and here and here. There is essentially nothing provided and nothing about those programs that is meaningfully related to the nature of problem substance use and its effective treatment.
The positive thing we can say about that $hugely profitable non-medical treatment industry is that it may be less lethal than the equally profitable medical substance use treatment industry, dispensing medications for an entirely non-medical condition of problem compulsive substance use. Described here in multiple (many) posts, medical “treatments” for substance use are a fiction, provide no benefit, and those alluded to in the article – buprenorphine and methadone – are established as fueling a worsening opioid crisis.
But what about the culturally-normed, iconic religious subcultures (Alcoholics Anonymous and Narcotics Anonymous) that essentially serve in popular media as stand-ins for substance use treatment? And by near universal consensus actually are and provide forms of treatment for SUD? So ingrained and enshrined as “treatments” or at least beneficial for substance use disorders that no American judge hesitates to mandate, on risk of life-altering punishments for non-compliance, participation in the programs? Despite every federal court ruling establishing that as a violation of the constitutional right of freedom from religious coercion? What about AA and NA?
It turns out that they are nothing other than what they appear to be – bizarre religious subcultures and whose prescriptions, practices, and directives predict harm, because they are countertherapeutic. That is, everything we know from decades of research in psychology, mental health, human development and behavior, is violated by the bizarre dictates of the 12 Steps and meeting practices, described here and here, for example.
All of that helps us understand why involvement in AA or NA comes with a probability of failure (continuation or return to problem, high-risk substance use) of 85 to 95 percent. Not something that can be conscionably promoted as “essential to maintaining sobriety“.
That means that for everyone like Devon, in our considered tale of disaster and community healing, 20 or more others engaging in AA or NA programming return to problem substance use. That probability of that failure not happening is likely less than the rates of “spontaneous remission” for substance use, that is, a higher risk of failure comes from participation than from problem substance users who have no involvement in AA, NA, or other treatments.
And Devon? We have no idea how he’s doing or how he will do, just that from the vefry sketchy account provided, he is a lonely person, and those meetings serve some social need for him. And that socially, in that “social network”, he will be exposed to peer pressure at those meetings to join others in use of traditional cigarettes, the preferred drug of the AA/NA subculture, encouraged and socially normed there. That habit and social network ritual is as likely as use of opioids to leave someone like Devon’s daughter without a father too early in her life.
A main benefit from the effects of Helene?
That occurred over the extended period when Devon was so engaged in managing his immediate stressors related to the hurricane and other parts of his life that he became free of the NA meetings, Free from being required to adopt an “addict” identity and submit to his “powerlessness”, instead using his competence and empowermennt to function well for an extended period, through some of his roughest challenges including divorce and custody determinations. Without any NA involvement and the imposed weakness and self-denigration that requires.
The worst of the effects for people “in recovery”?
Reinforcement of their weakness in the desperate, frenzied efforts to make sure they would not be deprived of their doctor-dispensed opioid drugs, the drugs that keep them dependent and weak, never free of the internalized lie that they have a disease only a medical treatment can help with, powerless and vulnerable through life and for the next natural disaster.
Let’s move on.

Not since Saddam Hussein was vilified, hunted down and hanged to helpfully avert Americans’ attention from the crimes of their celebrated, sociopathic elected leaders has there been as florid and necessary a public scapegoating as that of the excellent capitalists running Purdue Pharma, the evil Sackler clan. That concerted, effective, universally satisfying scapegoating (described here and here and here and here) has been necessary, of course, the alternatives horrifying and to be avoided at all costs – facing the obvious truths that the Sacklers and Purdue Pharma had nearly nothing to do with the opioid crisis as we know it, other than to supply America’s licensed medical professionals (LMP) and their patients with the opioids they were doling out and demanding.
You wouldn’t get that from the universal consensus media reporting over the past week or so as the legal dog-and-pony show dissipates, dominated by longstanding themes of justice finally done, of America – other than the Sackler family members – as victim, and of the sheer evil of it all, how this family could unimaginably have their pharma plants manufacture all that oxycontin that doctors were writing prescripitons for after having some very nice meals and other $payoffs from the Purdue pill salesmen. And after one of America’s top medical journals added a seminal single, meaningless note in a journal issue that became American Medicine’s permission slip to dose America with the addictive opioid, against all longstanding evidence. And after America’s medical institutions, hospitals, and governing bodies made it a professionally substandard behavior to not prescribe the addictive opioids. All detailed in the long-buried account by Sam Quinones, “Dreamland”. And by Chris McGreal in “American Overdose”.
Pudue Pharma obliged those medical demands.
But none of that really matters, at least not enough, not more than the need for a scapegoat to completely distract from and take the place of understanding how that demand for the effects of opioids, abused, was created, and created by whom.
That’s been understood for decades now, as the predictable effects of deficits in emotional regulation and self-management hence vulnerability to compulsive use of substances to moderate poorly managed, exaggerated emotions, those traits the products of childhoods in America’s families when children are exposed to psychological and emotional injury, to abuse and other forms of trauma, most frequently by parents, also by other adult family members and older siblings, rarely by adults outside of the family. That, as is well established, sets up those blameless children for high vulnerability to substance use and other problems.
That’s how it works and why the Sacklers must be burned at the stake. To avoid the horror of truth in a culture too sick to look at what it inflicts on its children.
In America’s Story, the Sackler family, conveniently, is the sole source of harm.

“Crisis is a necessary condition for a questioning of doxa, but is not in itself a sufficient condition for the production of a critical discourse.”
– Pierre Bourdieu Outline of a Theory of Practice (1972)
In Bourdieu’s Theory of Practice, heterodoxy is dissent, challenge to what “goes without saying” – the accepted, constructed doxa, “knowledge”, reality, that goes without saying precisely because it “comes without saying”, without real scrutiny, untested, unquestioned. The function of doxa is not knowledge or truth or promotion of the collective good, but to protect and serve the interests of those with the power, the cultural capital, to create it.






