OPIOID CRISIS CALIFORNIA: 8 MILLION+ DISTRIBUTED KITS, A HALF MILLION+ DEATHS PREVENTED WITH NALOXONE AS EMERGENCY HARM REDUCTION AGAINST LETHAL EXPERT TREATMENT FAILURE
As elsewhere, everywhere consistently, yearly increases in deaths averted by recorded and undercounted naloxone saves more than account for all reductions in deaths
by Clark Miller
Published April 10, 2026
The numbers from the Golden State are remarkable, astonishingly impressive, and a grim reminder of how intractably a worsening crisis of potentially lethal opioid high-risk use and overdose demands desperate emergency reversals of imminent deaths.
The AEDs of the opioid crisis, naloxone kits, of course, do not treat or provide gains against the underlying condition – compulsive, life-threatening, high-risk opioid use – instead are, like AED units, a measure of the severity of the underlying public health failure, of an American epidemic.
That AED analogy is more fully developed here and in numerous other posts at ACD and here, at Illness and Cure.
In California, it paid off … sort of. We’ll get to that.
With progressive, year-by-year dramatic increases in funding, supportive policy changes, distribution efforts, and community-based outreach and training, California became increasingly saturated with the AED analogs – death-preventing naloxone kits.
That had to reduce opioid deaths, and it did.
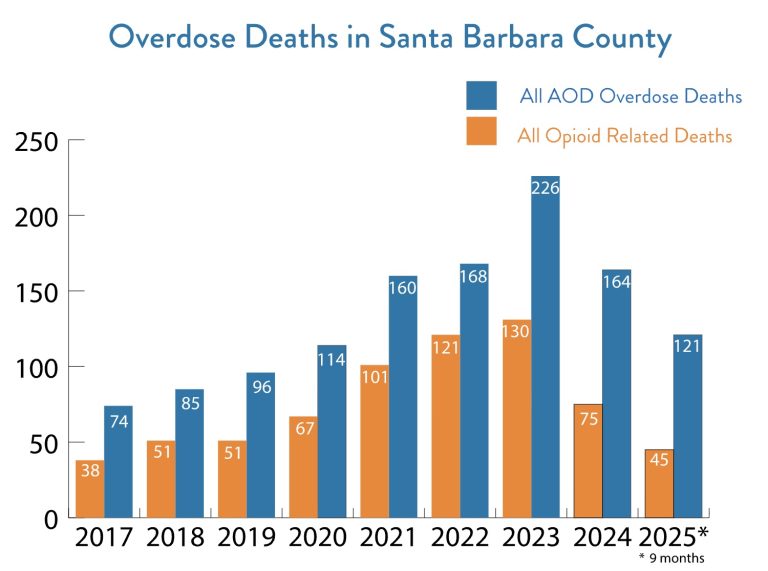
Santa Barbara County evidenced the same trend, the graphic reminding us that drug overdose death trends are not equivalent to “opioid-related” overdose deaths.
So … California.
In the constricted, incestuous, inbred world of opioid crisis constructed experts, trends in California have been understood variously, including as a “west coast” state imbued with “liberal” or “progressive” = “permissive” attitudes, cultural norms, and polices affecting drug use trends, California contiguous, after all, to the decriminalization state of Oregon.
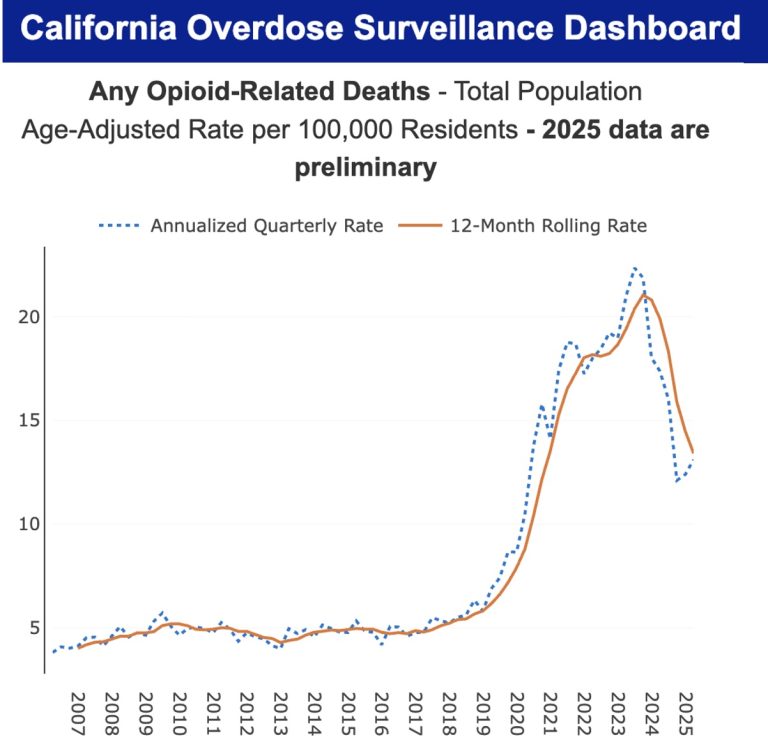
And yet, California’s relative delay to beginnnig of decreasing opioid overdose deaths occurred no later than many East Coast, Southern, and Great Plains states, and earlier than West Coast liberal, permissive bastions Washington and Oregon.
[Reminder: figures for “drug overdose deaths” are different, and greater, than for all opioid, synthetic opioid, or other subset of opioid deaths.]
Let’s start here, from an LA Times May 2025 story –
Shoshanna Scholar, director of harm reduction for L.A. County, said the key to saving lives is clear: Ramp up naloxone distribution and overdose prevention efforts in high-risk communities.
“Over the last 25 years, there’s been a real reckoning with substance use and seeing it as a chronic condition, as opposed to bad behavior that requires punishment in order to change it,” Scholar said. “We know there’s another path and it actually works to reduce the number of dead people.”
Since 2023, California Gov. Gavin Newsom has invested over $1 billion in grants for naloxone distribution, fentanyl test strips and other anti-overdose initiatives. Naloxone — also known as Narcan — is now available for purchase for all California residents through the CalRx initiative for $24.
[emphasis added]
For our valuable, very important interest in understanding the relationship between fatal opioid overdose trends and the use of naloxone to reverse otherwise fatal overdoses, some salient points emerge.
L.A. County’s director of harm reduction attributed in 2025 the shift (beginning 2023) to “saving lives” to a ramping up, an increase in naloxone distribution and use.
That distribution is targeted, as has been the case consistently in other widespread examples of effective naloxone campaigns, “in high-risk communities“.
The timing of what apparently has been a large infusion of state dollars toward that end started in 2023, directly antecedent to the drops in deaths.
From this source:
1. What are data reporting requirements for entities receiving naloxone through the NDP?
Entities participating in the program agree to maintain and report information regarding the number of reversals that occurred using the naloxone provided by the NDP. Please report reversals to naloxone@dhcs.ca.gov with each incident, or submit the total number of reversals using the previous shipment of naloxone with subsequent applications to NDP via the online form. Entities that are re-applying for the program are required to submit information about overdose reversals using naloxone received through NDP.
And from the same source –
Alternative Sources for Naloxone
1. What are some alternate sources for Naloxone?
DHCS’s NDP is not the sole or primary source for naloxone in California. Individuals will soon be able to purchase Narcan nasal spray over the counter. …
Naloxone is available to all Medi-Cal beneficiaries with a prescription. Additionally, many other third-party payers (e.g., Medicaid, Medicare Part D, and private insurance) cover naloxone, …
Naloxone can also be furnished by participating community pharmacists to individuals if applicable requirements are met.
In addition, counties have SAMHSA grant funding available, such as Substance Abuse Prevention and Treatment Block Grants (SABG), to provide naloxone.
Counties and cities may also have opioid settlement funding that can be used to purchase and provide naloxone to local communities.
[emphasis added]
From California’s Naloxone Distribution Project (NDP), the most recent figures –
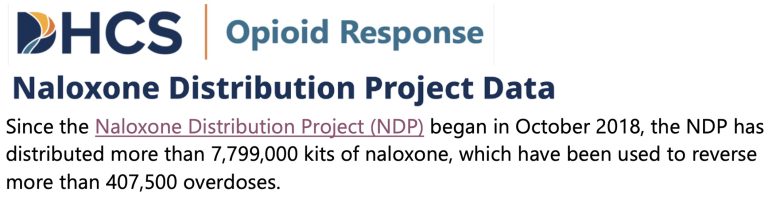
“distributed more than 7,799,000 kits of naloxone”
“used to reverse more than 407,500 overdoses”
Again, it’s important to consider that the estimates from the Department of Health Care Services (DHCS) represent only kits distributed by the NDP, not including additional units distributed by local community groups and organizations, like END OVERDOSE. Totals would be significantly higher.
It is important to understand that estimates of potentially fatal overdoses reversed are established as underestimates, as a large proportion go unreported and uncounted, as explained in detail here (and here).
Important as well, to consider that as of the estimates from DHCS in December of 2025, a couple of months ago, the state program had reversed –
“nearly 400,000 overdoses”
a jump by about 8,000 reversals over less than 2 months.
[UPDATE]: The DHCS continuously updates these estimates. As of March 4, 2026, the estimate for reversals associated with kits distributed by NDP only was slightly more than 410,000. We can be fully confident that beginning 2018 and considering all entities distributing naloxone along with the certainty of undercounts, as described, we are compelled to estimate potential opioid overdose deaths reversed as more than 500,000, almost certainly approaching 1 million.

Now, let’s rewind the tape and go back to August 2024. At that time the estimates provided by DHCS were:
“the state has distributed more than 4 million kits”
“saving more than 285,000 lives”
Then by April, 2025 the estimates of cumulative impacts:
“More than 6 million naloxone kits have been distributed to local governments and organizations since 2018
“About 355,000 overdoses have been reversed.”
Visualize the line graph for those numbers.
Let’s look at estimates of cumulative deaths prevented over the past approximately 18 months, beginning the year of overdose deaths starting to drop (2024), and for the earlier period spanning from when NDP began distribution (2018) up to August 2024, when opioid overdose deaths were finally dropping –
from NDP’s beginning in 2018 to 78 months later in August 2024, to a cumulative total of 285,000,
then from 285k to 355k over about 9 months,
then to 400k in 8 months or so,
then to 410k in another couple of months
Again, those are certain underestimates due to underreporting and only represent reports available to DHCS. Underreporting would have increased over the course of the intensive, targeted campaign as high-risk community settings became increasingly saturated and increasingly reversals would have occurred in peer, family, and layperson settings, without additional contact.
It bears emphasizing that estimates of potentially fatal overdoses reversed by naloxone are established as underestimates, as a large proportion go unreported and uncounted, as explained in detail here and in additional posts linked to in that post (and here). As targeted, layperson-based, intensive naloxone campaigns increased in successfully placing naloxone in the hands of community members, as in California and elsewhere, broadly, we can be confident that undercounts of reversals – that is, undercounts of high-risk use and overdose – have increased. There are powerful incentives in many, if not most, cases of overdose to not have contact with or have the overdose reported to professional services.

We need to further consider the available data and course of events in California.
We want to be able to compare, with the data we have available, magnitude of increases over time in increased use of naloxone to reverse potentially fatal opioid overdoses, by year, for example, compared to changes in prevalence of opioid overdose deaths over the same periods. We also want to know the magnitude of the reduction in the number of deaths.
Data available for this post allows us to compare best estimates of trends in numbers of deaths reversed by naloxone over the period 2018 (start date for the NDP) to August 2024 (first available estimate of cumulative total of “saves”), to the approximately 18-month period from August 2024 to the current date, March 4, 2026.
So far, so good? We are working with estimates and some assumptions. Please feel free to check the math as well.
Dividing the 285k (underestimated reversals) by 78 months over 2018 to August 2024 = 3.7k per month. For a one year period, that is 44.4k reversals on average over the approximately 6 years prior to opioid deaths decreasing starting in late 2023 to 2024. And prior to the dramatic changes in 2023 and into 2024 outlined above: the very large infusion of resources to intensify naloxone distribution and the appraisal in 2025, in retrospect, of those effects. Let’s review that.
Shoshanna Scholar, director of harm reduction for L.A. County, said the key to saving lives is clear: Ramp up naloxone distribution and overdose prevention efforts in high-risk communities.
“Over the last 25 years, there’s been a real reckoning with substance use and seeing it as a chronic condition, as opposed to bad behavior that requires punishment in order to change it,” Scholar said. “We know there’s another path and it actually works to reduce the number of dead people.”
Since 2023, California Gov. Gavin Newsom has invested over $1 billion in grants for naloxone distribution, fentanyl test strips and other anti-overdose initiatives. Naloxone — also known as Narcan — is now available for purchase for all California residents through the CalRx initiative for $24.
[emphasis added]
Now, where were we? Right.
For the period of August 2024 to the present, we have an estimate – from NDP only – of 125k saves. Per month, that’s 6.9k, and for an averaged 12 -month period, that’s 83.3k saves.
The difference for the two relevant periods is 83.3 – 44.4 = about 39k more saves per 12-month period over the more recent period, compared to pre-2024, and after the intensification in naloxone campaign efforts described.
Yes, there are assumptions and potential for error in these estimates, including that distribution and saves would have almost certainly been increasing to some extent over the “baseline” or “before” period of 2018 to August 2024.
So, from the start, let’s adjust our estimate conservatively to a difference of 30k. We’ll err on the side of underestimating and not overestimating the impact of year-to-year increases in naloxone-prevented deaths over the period of interest.
Okay, what about deaths due to opioids?
For lack of success in locating graphical representations or annual summaries of the drops in 2024 and 2025, I went to a source (CDPH Substance and Addiction Prevention Branch) of monthly estimates for California of monthly “drug related overdose deaths” for “Any Opioid”, here and here to find and selectively use a 12-month period that would correspond to the estimates we have for increases in naloxone saves post-2023, directly after “peak overdose year” for California, that is for a 12-month period beginning August 2024.
At this source, I found that total “opioid-related overdose deaths” for California in peak year 2023 were 7,847.
The sum of 12 months for August 2024 through July 2025 is 5,322.
The difference is 2,525 reduced opioid-related deaths comparing the periods of interest.
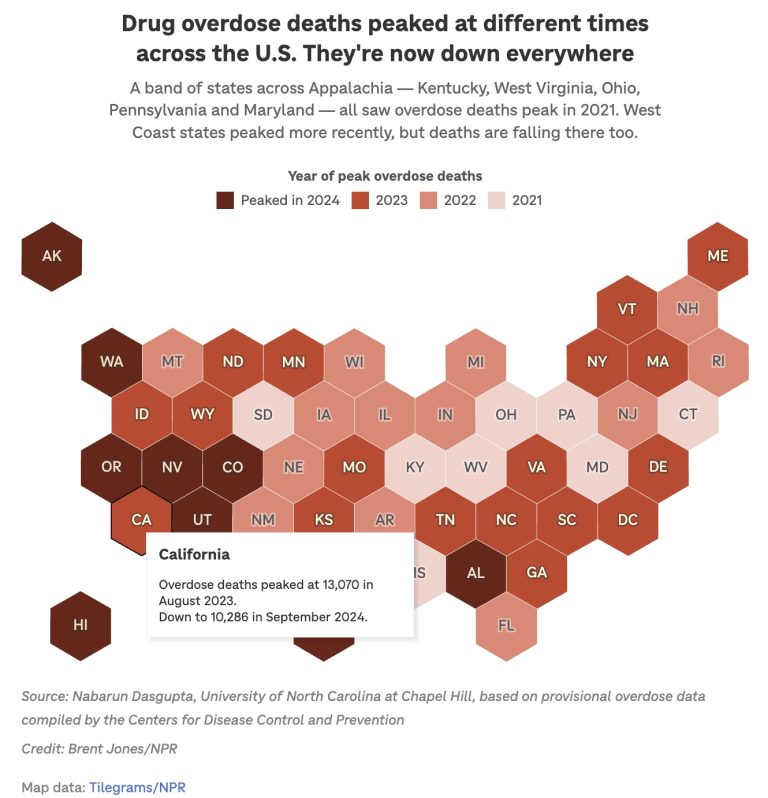
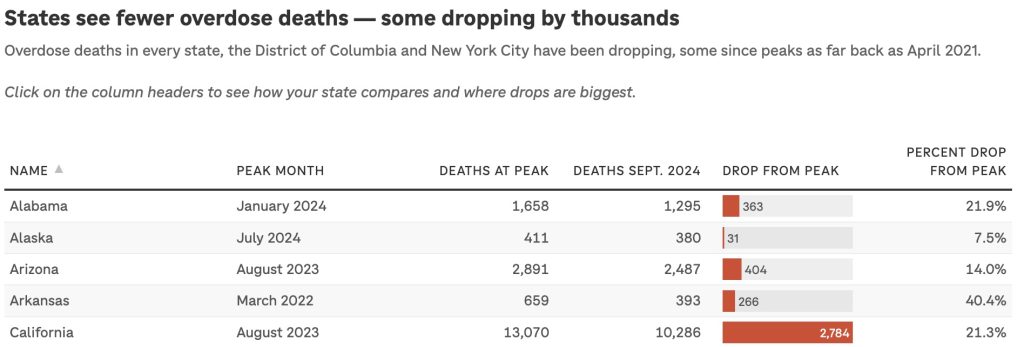
That corresponds well with, for example, the estimate of a decrease of about 2,800 OD deaths for all drugs from a peak in August 2023 to September 2024 (see the graphic for U.S. states above).
Now we need to think
We have already reduced our estimate of pre-/post- gain in naloxone reversals from 39k to 30k to account for there being an increasing trend over the pre- period.
Let’s err additionally on the side of avoiding an overestimate of naloxone effects.
A very real phenomenon that requires adjustments is that, increasingly, high-risk users are being revived repeatedly, up to potentially 10 times over a period of a year or 18 months, the period we used to estimate the increase in saves. Ten rescues over a period would not be common, and seems to be occurring. Use of multiple doses is not uncommon. We do not want to count, for one individual, multiple serial reversals each as a death prevented.
We could further lower our estimate to 10, 000 saves over the period of opioid deaths, dropping by 2,522, and the saves would be many more than needed to account for all drops in opioid-related deaths. That, it may be needed to be pointed out, leaves no reduced deaths that can reasonably be attributed to any other factors.
Let’s go a step further and reduce our estimate of 30k extra naloxone saves over the period of interest, and decrease it by an order of magnitude, to 3,000.
Same result, and we are compelled and obligated to draw the same conclusions.
Now, let’s get grounded again and remember that, as described and explained, due to known under-reporting of peer and layperson reversals and to our exclusion of any formal or informal collection of reversal estimates from all entities in California distributing naloxone other than the state’s NDP, that base estimate of 39k increase in reversals corresponding with drops in deaths is almost certainly a significant underestimate.
There is a “bottom line” here. This is it.
Given the data, related evidence, and factors we’ve considered, for any other factor to be legitimately considered as having significantly contributed to drops in opioid-related overdose deaths in California requires, with support of direct evidence, that the evidence we have considered to generate the estimated magnitude of increases in naloxone reversals cannot support those estimates. Without invalidation of those apparent increases in deaths averted by naloxone, the mystification of causes for drops in deaths must be seen for what it is.
For Baltimore, we used the same analyses and critical thinking to arrive at the same inescapable conclusions.
From that post:
Let’s get to the point
That figure of 18,000 reversals of potentially fatal opioid ODs (of fatal opioid deaths reversed) in Baltimore over 2015 to 2024 gives us some idea of the magnitude of death reductions due to emergency Narcan use. That would be about 1,800 for each of those years if there had been no upward trend, which we are essentially certain there has been.
But very roughly.
For the reasons discussed, they are a gross underestimate, the magnitude of the underestimate increasing over recent years.
Those figures are for just one source in Baltimore (“BDHD and its partners”), among all organizations engaged in naloxone campaigns.
But there’s a bottom line.
There were about 250 fewer opioid fatal ODs in Baltimore in 2024 compared to 2023, and then another 250 fewer in 2025.
For any factor other than emergency naloxone saves to have been significant in those recent year opioid OD death reductions, it is required to account for the data and evidence outlined in this post, and supported by additional evidence, to show that there were not year-by-year increases of at least 250 or more naloxone reversals for each of those years.
Lacking evidence to rule out those increases in reversals over 2023 to 2025, we are compelled to accept what seems to be almost certain – that emergency saves accounted for all of the fatality reductions, not other factors (and here).
That is, we are compelled to again acknowledge what has been apparent for years, that emergency naloxone saves have functioned as harm reduction against and have hidden the lethal failure of America’s expert gold standard treatment systems.

Back to our current post and to the new opioid crisis
In California, as everywhere, consistently (and here, and here) in the U.S. and Canada, persistently increasing high-risk opioid use and overdose, congruently with other valid measures, have incontrovertibly established the lethal failure of expert gold standard treatments, those treatments potentially effective only to the extent that they prevent high-risk use, the high-risk that’s been persistently increasing.
Saving a life is a good thing, and lots of lives are being saved by emergency rescues in California, as harm reduction against the established lethality of expert, gold-standard “treatments”.
Saved to engage in high-risk opioid use again, and again, in the absence of implementation of evidence-based (effective) prevention and treatments for compulsive substance use.
While serial Narcan reversals leave the survivors impaired and less able to engage in treatments, in the new opioid crisis.






