UPDATE ONTARIO CANADA: SURGING HIGH-RISK USE AND OVERDOSE IN A PROVINCE-WIDE WORSENING OPIOID CRISIS
Inside, outside of, and in areas without supervised consumption sites, by direct reports, high-risk opioid use and overdose are surging, ruling out drug supply, all other factors to explain death reductions – except naloxone
by Clark Miller
Published March 27, 2026
Let’s start, as seems invariably necessary, with the exposure and disposal of misinformation of the type driving persistently lethal epidemics.
“We did see a very similar drop in the number of overdose interventions that we’re doing, and Ottawa has seen a similar drop in the number of overdose deaths,” confirmed Rob Boyd, chief executive officer of Ottawa Inner City Health (OICH).
He said the downward trend is being seen across North America, in cities with and without supervised consumption sites.
While the reason for this decline remains unclear, front-line agencies in Ottawa say they haven’t noticed a similar drop in drug use. Boyd said that would suggest the drugs themselves are becoming less toxic.
[emphasis added]
“in cities with and without supervised consumption sites” (SCS)
It turns out those sites are not a factor in ways argued for or against, but in other important ways. We’ll come back to that.
And “that would suggest the drugs themselves are becoming less toxic“?
(Anyone who has kept up with trends in opioid and other illicit drug potency, variability, and risk, knows what to think about that and could skip over the following paragraphs to begin again at “Back to that CBC headline …”)
Less toxic than heroin and heroin/drug mixes in the decades before fentanyl appeared, with overdose deaths increasing by thousands yearly in a runaway epidemic? Were street drugs less toxic in a single locale in Ohio, not in contiguous and all counties in the state?
Let’s see what’s being reported related to “less toxic” drugs in Ontario.
In Windsor-Essex, a community without a history of SCS, as reported here,
An “increasingly toxic and unpredictable” drug supply is driving Ontario’s overdose crisis and has contributed to a recent spike in local opioid overdoses, the health unit says.
“Community partners report that some of the current drug supply may include beige or brown fentanyl with a dry, chunky texture,” the Windsor-Essex County Health Unit said in a news release.
“People who used these substances reported hallucinations and a very heavy nod, which may mean the drugs contain other depressants or contaminants.”
[emphasis added]
In Brockville, at least 50 miles from any supervised consumption site, a September 2025 news report headlined
“Brockville sees concerning rise in opioid overdoses”
describes increasing nonfatal overdoses and that –
Brockville Police and the South East Health Unit (SEHU) are alerting the community to an increase in overdoses in the community. …
“The unregulated drug supply continues to be highly toxic with high potency opioids and other central nervous and/or respiratory system depressants such as xylazine and benzodiazepines,” SEHU said. “Further, over the last few months, carfentinal is being detected in the drug supply in areas outside of Toronto such as Kingston, Peterborough and Thunder Bay.”
Carfentanil is a synthetic opioid 100 times more potent than fentanyl.
[emphasis added]
From an August 2025 report on trends in Ontario’s largest cities,
Guelph has seen “reports of escalated behaviours in the downtown core” since April, Wellington Guelph Drug Strategy manager Jean Hopkins said. …
More people are using alone, which increases risks and lowers the chances of getting people into care, she added.
“The unregulated drug supply continues to be highly toxic and unpredictable,” she said, noting that two public health alerts for high-risk drugs have been issued since May. …
Those working to contain the crisis are “losing ground,” Ottawa Inner City Health CEO Rob Boyd said.
The toxic drug crisis is unpredictable and can “change in an instant,” Boyd said.
“So I think people might be getting the impression that this is going away,” he said. “And it’s not.”
[emphasis added]
In Hamilton –
“We are essentially just sitting back and watching a crisis unfold in front of us,” said the NDP’s Dr. Robin Lennox, MPP for Hamilton Centre. “We’re likely just going to see this get worse and worse. …
“We’ve now systematically rolled back interventions meant to prevent overdose, like supervised consumption sites,” Lennox said. “Right now, we’re just at the whim of the toxic drug supply so when the drugs become more dangerous, we’re going to see more overdoses happening in our community.” …
However, it’s not just the number of calls that is raising alarm, but also the severity, said Mario Posteraro, president of OPSEU Local 256, which represents the Hamilton Paramedic Service.
“The resuscitations have become more prolonged and complex in the presence of other substances, which cause heavy sedation and are resistant to naloxone,” said Posteraro. “That means longer, more difficult and intense on-scene resuscitations.” …
“Since January of this year, there’s been an acute change in the drug supply where we’re seeing a resurgence of … benzodiazepines, as well as medetomidine, which is a veterinary tranquillizer,” Lennox said. “The combination of both of those substances in fentanyl is making people overdose at higher frequency and with more profound sedation.”
[emphasis added]
It’s important to digress to note the dangerous misinformation provided by the reported statement of Dr. Lennox.
In fact, SCS are specifically designed to provide, as needed, reversals of potentially fatal opioid overdoses by high-risk users bringing drugs they obtained on the streets to the facilities to use.
The only way to understand this statement in the news report is that by error or misunderstanding, her conveyance that SCS are meant to prevent fatal overdose was incorrectly reported as “meant to prevent overdose”.
And in Toronto –

Toronto Public Health is warning residents after a sharp increase in opioid overdoses was recorded in the city over the holiday period.
According to an alert issued by the agency, Toronto paramedic services responded to 122 suspected opioid overdose–related calls between Dec. 20 and Dec. 28. That figure is 35 per cent higher than the two-year average for the same time frame. However, this has not resulted in a rise in fatalities; public health officials say the number of fatal overdose-related calls during that period was under five. …
The alert also points to growing concerns about contamination in the unregulated drug supply. Toronto’s Drug Checking Service reports higher-than-usual levels of para-fluorofentanyl detected in fentanyl samples.
In addition, 81 per cent of fentanyl samples tested contained medetomidine, a veterinary tranquilizer that can increase the risk of overdose and complicate medical response.
[emphasis added]
So much for “less toxic” drugs on the streets of Ontario cities.
It’s important to add some background and context
From this August, 2025 news report –
On April 1, the Ford government effectively ended supervised consumption services at nine sites in Toronto, Hamilton, Ottawa, Guelph, Kitchener and Thunder Bay. The sites have transitioned into “HART hubs,” providing many of the same services they once did, minus drug use or needle exchanges.
Since then, overdose deaths have continued to slowly decrease, as they have since 2023 in Canada and the United States.
Back to that CBC headline and the necessary mystery it fabricates –
We know why. As does anyone following the reports, data, and forensic evidence, and who doesn’t mind thinking about it.
It’s outlined in this recent post for another Ontario community, Hamilton.
The CBC report for Ottawa wrongly conflates and confuses fatal opioid overdoses with nonfatal, a profoundly distorting and muddying confusion that allows expert/media collusions to avoid the meaning of the distinction.
We’ve just dispensed with the remarkable attribution of recent-year drops in opioid OD deaths to a less toxic drug supply. Cover stories that attribute those drops to opioid supply disruptions or shortages (e.g. “supply shock“) are also dismantled and nullified, including here and here and here and here, here, and here.
From that recent post explaining trends in Hamilton, Ontario and explaining how we are confident that – as everywhere, consistently – it is entirely the desperate, increasingly targeted and effective, intensive naloxone campaigns that account for drops in opioid OD deaths –
Here’s what all of that looks like –
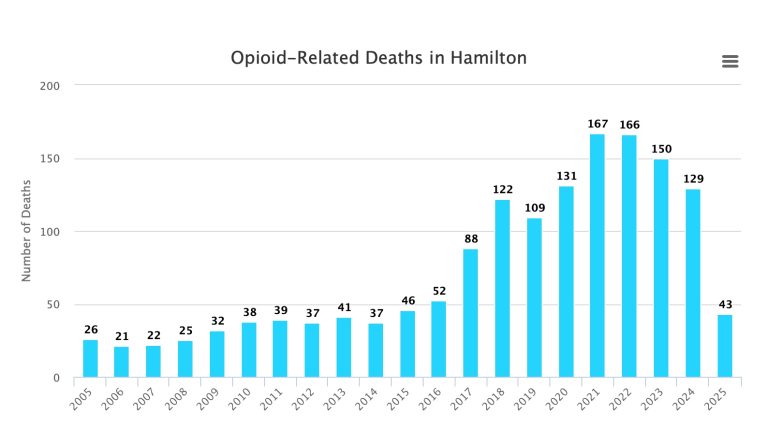
Hamilton and province Ontario following similar patterns
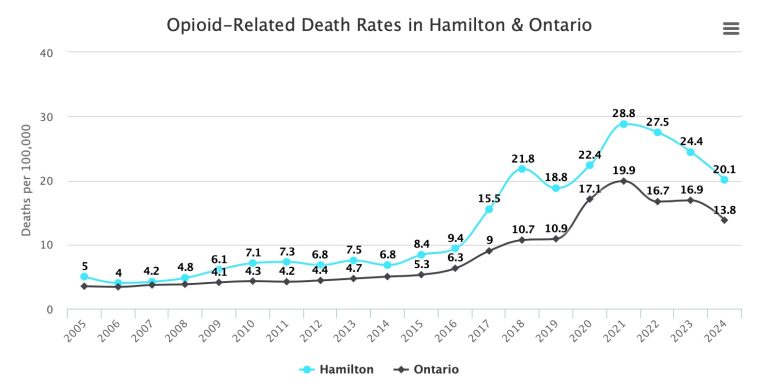
And predictably, a tight temporal correlation with public availability of naloxone, distributed for use to reverse potentially fatal opioid overdoses.
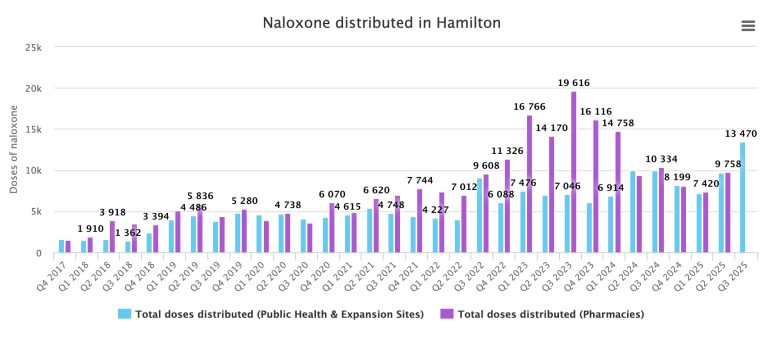
Comparing the graphics, it’s important to note –
The difference in timescale for naloxone distribution
That total naloxone distributed is the sum of each pair of differently-colored bars each quarter
That naloxone distribution was to sites (pharmacies, community programs, public health) directly providing units to laypersons (opioid users, their families, peers and friends), not law enforcement or first responders and
Naloxone distribution surged from late 2022 through 2023, remaining high thereafter, corresponding to initiation of and sustained dramatic drops in opioid deaths through 2024 and 2025
Back to our currrent post –
And back to our lead news report from the CBC about opioid overdoses and fatal overdoses in Ottawa, Ontario –
“We did see a very similar drop in the number of overdose interventions that we’re doing, and Ottawa has seen a similar drop in the number of overdose deaths,” confirmed Rob Boyd, chief executive officer of Ottawa Inner City Health (OICH).
He said the downward trend is being seen across North America, in cities with and without supervised consumption sites.
While the reason for this decline remains unclear, front-line agencies in Ottawa say they haven’t noticed a similar drop in drug use. Boyd said that would suggest the drugs themselves are becoming less toxic.
[emphasis added]
“… front-line agencies in Ottawa say they haven’t noticed a similar drop in drug use”
Now it gets interesting, the distinctions and their meanings.
Naloxone, of course, is. not able to benefit by stopping or decreasing high-risk opioid use, does provide clear benefit by reducing the frequency at which high-risk use and overdose result in fatal overdose, in fact is established as being solely responsible for recent, significant reductions in overdose deaths in the U.S. Some would contend that its use enables, even facilitates persistent high-risk opioid use, and it is difficult to argue against that, not possible to argue ethically against its continued use.
All other treatments, interventions, public health policies, and fabricated explanations for recent drops in opioid OD deaths are distinctly different. Traditional “addiction treatment”, medical substitute opioid treatment, other interventions potentially have benefit and prevent opioid deaths only by and if prevention of high-risk use and overdose occur.
That’s different.
That’s how we know that the iatrogenic opioid crisis is worsening, because decades of medical and other gold standard cures have failed to reduce high-risk opioid use, necessitating desperate, intensive naloxone campaigns to moderate their harm.
And in Ontario, Canada? It turns out that CBC headline, up at the top of this post, is lethally sloppy, benighted, harm-predicting, because as we’ll see, the evidence points to the confident conclusion that opioid high-risk use and overdose are not deceasing, instead increasing in the province, reflecting expert treatment failure that must be desperately moderated, as everywhere, by intensive naloxone campaigns that reduce deaths and hide the gravity of a worsening crisis.
Let’s take a look at those increases in high-risk opioid use and overdose
Back to Toronto, where opioid overdoses were surging as measured by paramedic responses late last year. That could be a reflection of the effects of closure of some of the city’s SCS earlier last year, shifting significant portions of naloxone reversals to public places. But, the remaining SCS were overwhelmed by increases in overdoses in their facilities as well, reported in the news video here.
In Toronto, reported here, direct reports of drop-in centers (as distinct from SCS) point to a
“staggering” increase in overdoses, an indication that more people are choosing to use outside of the remaining sites
That conjecture that high-risk users unable to use a SCS that’s been shut down are in large numbers “choosing to use outside of remaining sites” is not consistent with reports that remaining SCS have been overwhelmed as well with overdoses.
A factor that independently points to generalized increasing high-risk opioid use and overdose in Ontario is the timeline.
Multiple SCS in Ontario were shut down in March and April of 2025. It’s reasonable to expect that some displacement of users at those sites would be evidenced by increases in medical emergency naloxone overdose reversals in the adjacent areas and in remaining SCS, but that would happen immediately and tend toward a new baseline or equilibrium in locational distribution of overdose and reversals, over a period of weeks or at most a few months after the disruptions. Those changes would reflect disruptions due to the closures, and not overall increases in high-risk opioid use and overdose in the province.
But increases in opioid overdoses persisting and occurring past a few weeks or a month or so after the closures cannot reasonably be attributed to the adjustments users would have had to make in the days and weeks after closures.
So, for example, the surges in overdoses in Toronto in November and December of 2025 cannot be accounted for in that way, and must reflect generalized increased high-risk use and overdose.
Nor can those in Brockville, reported here, in September of 2025.
Nor can the surge in high-risk use and overdose as reported here for Windsor-Essex, a community without a history of SCS, be attributed to SCS closures a year prior in distant areas of the province.
Between Feb. 22 and Feb 28, Windsor-Essex emergency departments recorded 19 overdoses, 16 of which involved fentanyl. Local shelters also reported “drastic” increases in the number of overdoses they’ve responded to in recent days
The unusually high number prompted an alert from the health unit and an “urgent” meeting of dozens of community partners on Tuesday afternoon.
Nor can a surge in opioid overdoses in Ottawa in the first two months of 2026, as measured by emergency responses of Ottawa Police, be attributed to shifts in the location of opioid overdoses that would have been made immediately after users needed to adjust to the closure of an SCS in the Lowertown West neighbourhood in September 2025. Those changes would have occurred in the days and weeks immediately after the closure.
But so far in 2026, numbers seem to be climbing. Most recent year-to-date data encapsulates Jan. 1 to Feb. 17. In this time period, OPS responded to 93 overdose calls, compared to 51 during the same period in 2025.
That news piece highlights an established and very important consideration for all analyses of opioid high-risk use and overdose trends. As desperate, intensive, community and layperson naloxone campaigns have placed kits in the hands of more and more peers and other community members, fewer and fewer reversals (= instances of high-risk use) are reported.
Ottawa saw a stiff decrease in the number of 911 calls related to overdoses in 2025, but police say that doesn’t always give an accurate representation of the problem across the city.
While the high rate of overdoses in the neighbourhood cannot be said to be a result of the closure of the site, it does represent a need for continued health intervention.
[emphasis added]
That’s an understatement, based on consistent reports in the province –
From Hamilton, in this report –
Many overdoses go unreported due to the prevalence of the overdose-reversal drug naloxone, meaning the real number is likely higher, Richardson said.
From Ottawa, in this report –
“The data provided by paramedics is just the tip of the iceberg because we know that peer workers and just regular, everyday neighbours, and also our ANCHOR non-police crisis service have also been reversing overdoses,” Troster said. “What’s captured in the paramedic data shows a trend, but it’s actually a much deeper trend that we’ve been seeing since the first day that the consumption site was forced to close.”
Back to nonfatal overdose trends in Ontario and SCS closures
Any such readjustments to SCS closures early last year (2025) that would have necessarily resulted in immediate adjustments by users accessing an SCS and in locational increases that reflect locational shifts in overdose reversals clearly can’t account for a continuing surge in opioid-related overdoses in Hamilton, as reported March 12, 2026. Especially when increases are occurring both within a remaining SCS and in the community.
Hamilton was featured in this recent post. Let’s take another look.

Paramedic calls for opioid overdoses increased by nearly 40 per cent in one month to set a troubling record of more than seven a day in Hamilton.
The staggering rise to 199 opioid-related paramedic calls in February demolished the previous record of 143, set the month before despite January having three extra days.
“We are essentially just sitting back and watching a crisis unfold in front of us,” said the NDP’s Dr. Robin Lennox, MPP for Hamilton Centre. “We’re likely just going to see this get worse and worse.”
But it’s not just the paramedics seeing surges in overdoses, in Hamilton that’s happening in the remaining SCS as well, following the closure of one site in March of 2025.
Nine overdoses were reversed just in the week leading up to March 9 solely at the YWCA’s Safer Use Space program on MacNab Street South, which Uppal said is much higher than usual.
In total, 124 overdoses have been reversed since April at that site, as well as at the YWCA emergency treatment program. Neither program has experienced any deaths. ..
The YWCA has been able to continue offering a safe consumption site for women and gender-diverse people, partly because it doesn’t depend on provincial funding. It’s also awaiting the outcome of an injunction that’s part of a court challenge of the province’s restrictions on supervised consumption sites.
[emphsis added]
That is, the surges in opioid overdoses are generalized, occurring at and outside of SCS, and far past any time frame over which the immediate displacement and adjustments of high-risk users to the closure of one site in Hamilton can account for, as discussed.
And fatal opioid overdoses in Hamilton are not increasing, instead have been on a decreasing trend.

It is important to remember that SCS do not prevent overdoses, are, in fact, designed to provide immediate naloxone (or oxygen) reversals for the overdoses expected to occur there, the reason for their existence. The high-risk opioid users coming in with street drugs to use at an SCS are obtaining the same “really dangerous”, “toxic” supply of drugs as other users in Hamilton.
“Since January of this year, there’s been an acute change in the drug supply where we’re seeing a resurgence of … benzodiazepines, as well as medetomidine, which is a veterinary tranquillizer,” Lennox said. “The combination of both of those substances in fentanyl is making people overdose at higher frequency and with more profound sedation.”
There are no surprises here, in these reports for Ontario, Canada, any more than there are for the persistently worsening opioid crisis in the U.S.
The dramatic, emergency, successful naloxone campaigns reducing fatal overdoses, necessitated by persistently surging high-risk opioid use and overdose, are predictable from and a reflection of the lethal failure of medical and other gold standard expert “treatments”.
Back to Ontario
Reported here, in London, Ontario, where the only SCS site is still open –
Meanwhile, in London, Ont., police issued a public safety alert in early March after authorities handled 39 overdose-related emergency calls in a 24-hour period. London’s only safe-consumption site – which stopped 218 overdoses last year – is set to lose its provincial funding in June 2026.
And reported here, in Toronto, nearly a year after closure of some SCS sites –
In Toronto, overdose-related emergency calls have been climbing since the fall. In January 2026, paramedics recorded 350 non-fatal suspected opioid overdoses in the city, an increase of 47 per cent over the previous January.

TAKEAWAYS
In Ontario, Canada, increases in opioid high-risk use and overdose are generalized and province-wide, reported within supervised consumption sites, outside of them in public spaces, on timelines that rule out increases due solely to adjustments of high-risk users to SCS closure, in areas without a history of SCS, and in areas with SCS and no closure.
Fatal opioid overdoses have been declining, attributable, as everywhere consistently inn North America, to naloxone campaigns entirely.
The trends, as consistently in the U.S., highlight the established lethal roles of failure of expert gold standard treatments to effectively treat and curb high-risk substance use.
Serving as a highly resourced and facilitated form of emergency naloxone overdose intervention, like distribution and training efforts, SCS does not address high-risk use and overdose, does save lives, and hides the lethal failure of expert treatment approaches.
Reliance on naloxone as harm reduction against gold standard treatment failure is a lethal dead end, contributing to a worsening crisis.






