ROUNDUP – OPIOID OVERDOSE DEATHS RISING; CONFUSED, EXPERT-WANNABE AUTHOR PROMOTES NEW WAR ON DRUGS IN THE WaPo; DRUGS WIN IN WAR ON DRUGS
Official claims of millions of lethal opioid doses taken off the streets can only be credited with reducing deaths if high-risk use and overdose are decreasing. They are not. It’s the Narcan.
by Clark Miller
Published April 17, 2026
From an area in Washington we are familiar with as described in this recent post, predictable, unsettling news from adjacent counties –
Fentanyl continues to be a scourge on the Tri-Cities, driving the number of overdose deaths to new heights. Overdoses were responsible for killing 89 people in Benton and Franklin counties last year, according to coroner reports. That makes it the single largest cause of accidental deaths and is nearly 40% higher than in 2024.
The increase is driven by fentanyl.
The synthetic opioid played a role in more than two-thirds of last year’s drug deaths. …
Normally, the health district looks at the rates of overdose over the population, and are seeing the rates are still trending upward. That means it isn’t being driven by a growing population, explained Kelly Harnish, the district’s healthy living program manager.
“The crisis is less about one substance and more about fentanyl entering an increasingly mixed drug supply,” Harnish said. …
The way people are taking fentanyl is changing as well.
It’s becoming more common for it to be sold as a powder. This is often mixed with other drugs, such as methamphetamine.
Those persistent increases in opioid overdose deaths have come despite intensive law enforcement interdiction efforts.
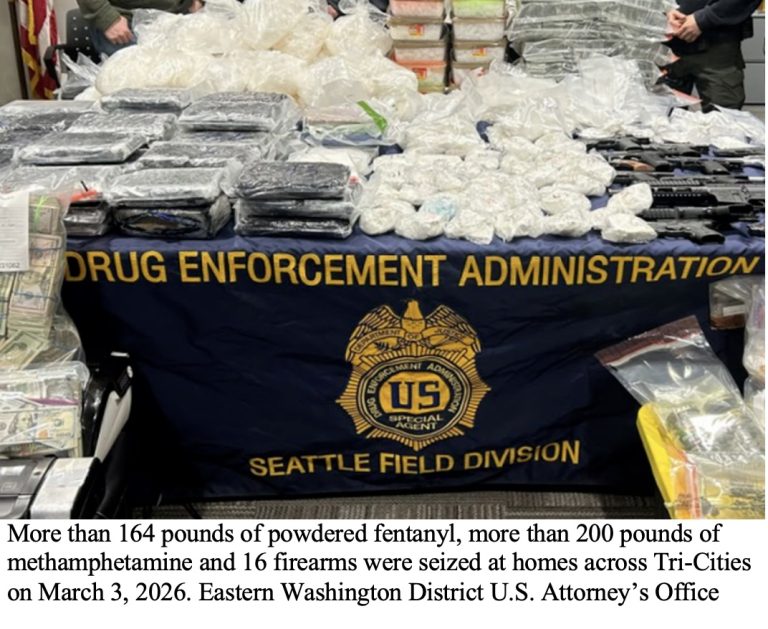
Huh! That seems like a lot of fentanyl for a rural three-county area with a combined population of approximately 420,000.
And it’s not that DEA supply disruption efforts have been late in coming.
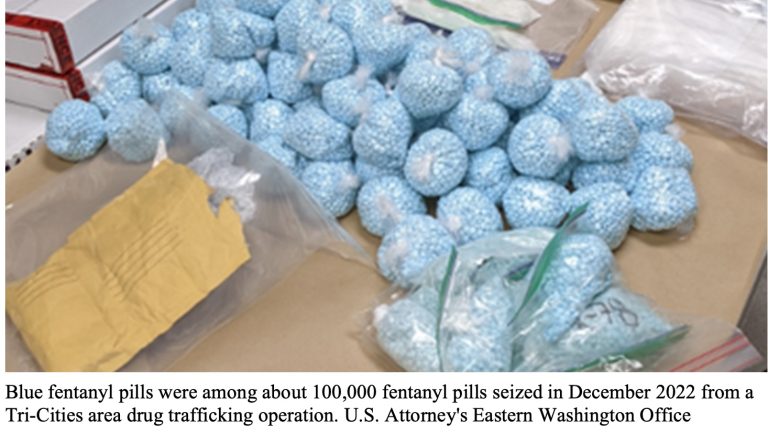
Reported here, in late 2022, the DEA confiscated “more than 100,000 fentanyl pills” in the area along with other drugs and weapons. Their coordinated Tri-Cities war on drugs had begun as early as 2020, reported here.
In 2023, follow-up investigation led to the seizure of an additional 238,000 fentanyl pills, reported here.
From additional local reports, the fentanyl has been destined over past years for sales in the Tri-Cities and surrounding areas.
Based on the sizes of those enforcement and seizure operations, in a rural area of less than a half-million population, that would have to be considered a major supply disruption, wouldn’t it?
And if our trusted leaders and authorities are right, those enforcement disruptions have been very effective in reducing opioid deaths.
But it’s not just that. A popular opioid crisis author turned expert has concluded that it is, in fact, legal interdiction of opioid supply chains that provides a way out of the opioid crisis, not prevention or addressing the conditions driving high-risk users to compulsively use drugs (demand-driven).
The example we started with, of opioid deaths continuing to surge over past years, at the same time that DEA coordinated seizures were taking very large quantities of fentanyl off the illicit market, seems to invalidate their claims.
But who knows! Maybe this example is an exception, a fluke, maybe we’re missing something.
Let’s keep exploring.
Let’s see if they’re right.
And that requires an initial digression.
Imagine the very common case of a high-risk opioid user, having administered an illicit substance that was believed to provide the needed relief from impending “dopesick” withdrawal symptoms and from the physical, emotional, and psychological pain and fears that drive all compulsive substance use.
This time, as is common and unintentional, the dose; potency, or makeup of what was taken is too much, more than desired, and the user is headed toward a likely fatal overdose, with the classic signs.
There is one type of intervention now that can prevent that death – one only – the urgent administration of naloxone or similar opioid antagonist, or oxygen in a supervised consumption site.
But wait! Let’s see, what else, though, after the potentially fatal dose has been administered, could reverse that impending fatal overdose? Medication assisted treatment with substitute opioids (MAT, MOUD, etc.) ? Fentanyl test strips? Addiction treatment? Fentanyl supply disruptions?
Yes, I know.
And yet, it is entirely necessary to be facetious, obnoxiously so, because the point has been lost, the most obvious point ever.
For each and every one of those “treatments”, interventions other than naloxone, harm reduction strategies, or supply disruptions, the only possible way to have benefit, to prevent fatal ODs, is to prevent high-risk use and overdose in the first place. And? If high-risk use and overdose are not demonstrably being prevented by them, then no reduced overdose deaths can be attributed to them.
Take just a couple of minutes to think about that. That is all that is required.
Now, where were we?
Right, our confused, expert-wannabe author providing expert treatment advice for an epidemic in the Washington Post.

As evidence, Quinones starts with an anecdote, one person, “a Salt Lake City woman addicted to fentanyl”, who conveyed to him that over a period of instability in street drug supplies (have there been significant periods of stability over the decades of a worsening epidemic?), she “sought treatment”.
She sought treatment.
Let’s imagine that she found herself accessing “treatment” For anyone remotely familiar with America’s addiction treatment systems, that establishes that her odds of NOT returning to high-risk opioid use were about 1 in 10, about 10 percent.
Quinone’s anecdote would have had the same cogency and import if it had been that the woman “started going to meetings” or “got a sponsor and “gave it up to her higher power”.
Here’s where Quinones went with that anecdote and the DEA-alleged changes in illicit opioid supplies –
“That shifts in the supply could have produced such a massive turn in fortune doesn’t surprise me.”
Mr. Quinones does not further describe that “massive turn in fortune”.
The major media piece is rife with misinformation, distortions, and most of all, the profound incapacity to form cogent, informed thoughts about compulsive substance use and its treatment and prevention.
There is a second anecdote at the end of the piece. Additional evidence from the writer.
Last year, I spoke with a woman who was addicted to the drug in Tucson, two hours from Mexico and a major drug through-point. Supplies of fentanyl had dropped mightily since a peak in 2023, she said, when pills cost between 50 cents and a dollar. Those pills now went for $5.
In 2022 and 2023, she overdosed 26 times in 15 months, revived each time with Narcan. But during her latest episode of drug use, she said, she hasn’t overdosed once.
Get it? Over a recent period, she has not overdosed, “during her latest period of drug use”. That is, she is still engaging in illicit opioid use, that is, high-risk opioid use, and over a period of unspecified duration, if she was telling the truth, she did not have an overdose.
That’s the evidence, conveyed in the Washington Post, supporting the new war on drugs.
Fortunately, there is real, valid evidence bearing directly on this very question.
Let’s consider it.
Changes and differences in incidence of fatal opioid overdoses are always confounded by increasingly prevalent, intensive, and successful naloxone campaigns and always have been. Idiocy notwithstanding, drops in opioid overdose deaths can never be attributed to factors other than reversed potentially fatal overdoses (i.e. to naloxone campaigns) unless naloxone use is ruled out and overdoses are decreasing correlated with the factor.
That’s a challenging goal, in the context that recent, nearly nationwide drops in fatal ODs are established as entirely attributable to naloxone campaigns and not other factors as in, for example, California.
High-risk opioid use, as indicated by overdose and reversal, is a valid measure of the severity and direction of the crisis, but increasingly and grossly qualified over recent years as effective, intensive naloxone distribution camplaigns have led to surges in reversals by peers and laypersons, reversals that don’t get reported in retrievable ways, that is, result in undercounts of overdoses = undercounts of high-risk use = underestimate of failure of gold standard treatments, supply changes, and other factors.

We can rule out
the presumed or fabricated benefit in reducing opioid deaths from enforcement or any other supply disruptions, from gold standard “treatment”, from any factors other than emergency agonist reversals of potentially lethal overdoses, because opioid high-risk use and overdose are continuing to rise or are not moderating. Everywhere.
That’s established by consistent reports across diverse locales in dozens of posts here and here, and is established by the immense and growing body of reports of precipitously surging numbers of potentially fatal overdoses prevented by emergency naloxone saves. Without surging high-risk use and overdoses, those campaigns would never have been necessary. They are harm reduction for the lethal failure of expert, gold-standard treatments.
Drugs are winning the benighted war on drugs, everywhere,
the lethal failure of expert treatments and approaches to prevent or treat compulsive substance use driving increasing high-risk use, overdose, and fatal overdose in the Tri-Cities area, Washington, as we saw, despite major interdiction and supply effects.
And in Rhode Island
And in Montana, where fentanyl in street drug samples had diminished significantly
And in Pittsburgh and Allegheny County, Pennsylvania, where fentanyl supplies were significantly disrupted, as described in the upcoming post: “THE LETHAL ROLE OF ABDICATION OF THOUGHT IN A WORSENING OPIOID CRISIS”
And as reported in Austin and Travis County, Texas, where opioid overdose death reductions are accurately attributed to naloxone, and “We know for a fact that the overdoses are still happening”.
Failing everywhere.
It’s the Narcan, providing harm reduction against lethally failed expert treatments on a dead-end road.
The rest is ruled out as ineffective and worse, despite the lies and mystifications.
Ruled out as having any benefit, yet persistently protected, persistently lethal.






