PARENT OPIOID ABUSE HARMING MILLIONS OF KIDS, THEIR FUTURE RISK HIDDEN AND BETRAYED BY EXPERT FICTIONS
Have kids traumatized in opioid abusing families been “scared straight”? Or set up to be at higher risk of dangerous drug use?
by Clark Miller
Published May 22, 2026
Here’s where the evidence-free fabrication may have started, with the comments of a constructed opioid crisis expert in this NPR piece in June 2025 –
“According to Dasgupta at the University of North Carolina, years of devastation caused by fentanyl and other opioids might mean more people in their teens and twenties are choosing to experiment with less risky drugs.”
That is, those affected or traumatized kids have been “scared straight”, or at least “scared safer”. That, despite the same expert noting that, in fact, for youth who were ages 13 to 19 in 2024, the year of the pronounced, highlighted drop in OD deaths –
“Some teens and 20-somethings are seeing far fewer deaths, but he identified one cluster born between 2005 and 2011 who actually saw a slight uptick in deaths over the past two years. The increase is relatively small — about 300 additional fatalities nationwide over two years — but Dasgupta said it’s an area of concern that needs more study to determine why.”
The conjecture was nevertheless expanded on in a news piece in the publication “PubliCola” in November 2025, highlighted and discussed in this post on Seattle’s opioid crisis trends.
From that post –
[sections italicized to emphasize]
The evidence so far is not cooperating with expert cover stories. That requires additional mystification, of the type mastered and employed in NPR reports, as here and here and here and here.
From the same PUBLICOLA report –
Dasgupta, who worked with harm reduction experts in Seattle while conducting his research, says the decline in Seattle’s fatal overdose rate is likely the result of four trends that are happening across the country. First, he says, illicit drug manufacturers are making the drug supply less toxic by improving quality. “This is a market correction, independent of any law enforcement action,” Dasgupta said.
Second, Gen Z is less inclined to use opioids than its predecessors. “We have a million and a half kids who lost parents, uncles, aunts and grandparents to an overdose in the United States,” Dasgupta said. “That experience of going to those funerals, I guarantee you, is way more likely to change their behaviors and attitudes towards opioids than any educational campaign.”
Third, Dasgupta said, drug users have learned not to use alone, and when they have the resources available, to get their drugs tested for potency.
And fourth, Dasgupta credits “all the community-based interventions that are going on. Clinic-based interventions have greatly expanded availability of addiction treatment as well as naloxone, especially having that be accessible with as little red tape as possible.”
[emphasis added]
“Dasgupta” is Nabarun Dasgupta, a researcher at the University of North Carolina, whose thoughts on opioid crisis trends are featured in posts here and here.
Astute readers will notice that naloxone – the one factor not only supported by evidence, but direct, incontrovertible evidence of accounting for fatal OD reductions – is added at the end, as an afterthought.
Let’s take a look!
“making the drug supply less toxic by improving quality”
Please take a few minutes for an internet search for ongoing trends in purity, toxicity, and instability of the illicit opioid street supply and any concerns related to that.
Right.
There is no evidence offered here and none available to support this conjecture helpful distraction. Nor is there evidence to support that to whatever extent there may be such an effect, it is causally related to a single reduced opioid overdose death. Fentanyl seems to be lethal enough without being more clean.
“Gen Z is less inclined to use opioids”
There is no evidence offered here and none available to support this conjecture helpful distraction. Nor is there evidence to support that to whatever extent there may be such an effect, it is causally related to a single reduced opioid overdose death.
In fact, on the supposition that disturbing, emotionally jarring and injurious experiences of the type pointed to are having effects, we know, it is established, that just the opposite effects are predicted.
Growing up in a household affected by drug use, overdose, and associated psychosocial and developmental stressors is the strongest predictor we know of for future problem drug use.
“drug users have learned not to use alone”
That is true, covered in numerous posts at ACD, and points directly to the role of naloxone in decreasing fatal overdoses.
And, “when they have the resources available, to get their drugs tested for potency.”
For high-risk, “street” opioid users and for almost all users, this does not warrant comment. It is sufficient to note that if control of purity and potency were, in practice, protective factors, then there would be some evidence to support benefit from “safer supply” approaches rather than their established lethality.
“expanded availability of addiction treatment”
There is no evidence offered here and none available to support this conjecture necessary distraction.
Back to our current post.
That unsupported claim (along with the invalidated supply disturbance fabrication) was repeated, reported here, by a panel of medical and academic opioid crisis experts, in February of this year.

In a Feb. 13 panel hosted by the Leonard Davis Institute of Health Economics (LDI), researchers in addiction medicine, policy, and behavioral science said the recent decline in fatalities likely reflects a combination of fentanyl market changes, expanded naloxone and treatment access, and fewer young people initiating opioid use after witnessing devastation among other household members. But the panelists warned that focusing on overdose death statistics alone masks broader persistent suffering, widening disparities, and severe morbidity from new street-drug adulterants such as xylazine and medetomidine among living users.
[emphasis added]
Let’s go back a few steps to examine the first of two parts to this unsupported fabrication – that adolescents, teens, and young adults, an age group growing up during the height of the opioid crisis and exposed to ACE, family dysfunction, and potentially traumatizing events in their families related to high-risk opioid use by parents or other adults, have become less likely to engage in high-risk opioid use themselves and to overdose.
Is it true that “Gen Z is less inclined to use opioids”?
There are some things we know that apply to that question, and a lot we don’t know.
As described in detail in this post, at least one of the major, yearly surveys experts have marshaled to paint a picture of significant gains in reductions in youth substance use, neglected to include “opioid” or “fentanyl” among substances respondents were asked to self-report on.
What we know with certainty is that those national surveys are, in any case, invalidated, explained here and here.
Invalidated due to selection bias, in these cases by excluding youth most at risk for problem substance use from taking the survey (explained here).

And invalidated for the selected, biased subpopulation of regular high-school attendees, by conditions of the surveys and environments that confidently predict underreporting, explained here.

That is to say, high-risk or problem opioid use by teens and young adults was not validly or meaningfully measured in the national surveys experts have relied on to characterize youth substance use trends.
We can conclude with confidence that problem opioid use was grossly underreported and underestimated in those surveys.
So, what do we have to go on?
There’s this, from this source (with citation):
“Between 2018 and 2023, rates of opioid-related deaths in US adolescents ages 12–17 increased approximately 280 percent, while increasing 65 percent in adults.1”
And this, from this CBS news piece:

The “exposure” identified as “misuse or drug abuse” increased markedly, separately from “unintentional” exposure.
Cases of fentanyl poisoning in children across the U.S. has been steadily increasing for most of the past decade, according to a new study published Friday.
Researchers looked at over 3,000 incidents of nonfatal fentanyl exposure in children up to 19 years old that were reported to poison centers, and found a 1,194.2% increase between 2015 and 2023, according to the study published in the American Journal of Drug and Alcohol Abuse.
The exposures were categorized as either misuse or abuse, or as unintentional. During the studied period, the percentage of misuse or drug abuse cases increased from 26.1% to 39.2%, while there was a decrease in unintentional exposures, from 47.8% to 35.4%. ..
The majority of fentanyl exposure cases among teens, 65.7%, were characterized as intentional misuse or abuse, the study’s authors found.
[emphasis added]
And there’s this new study, presented at the Pediatric Academic Societies (PAS) 2026 Meeting, April 24-27.
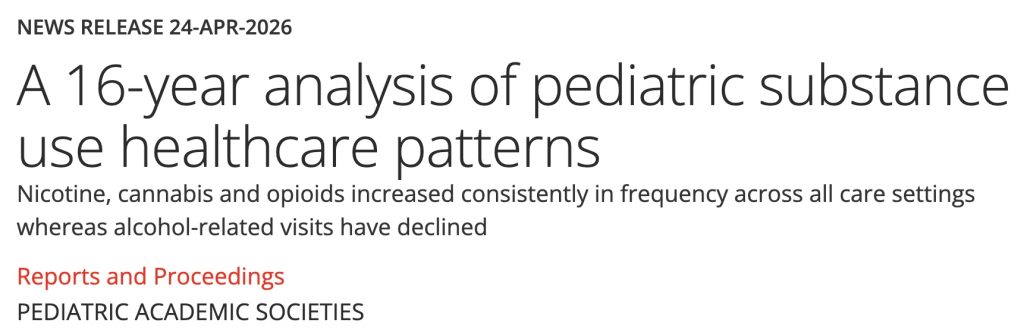
BOSTON, April 24, 2026 – Over the past 16 years, pediatric substance use-related visits (SUVs) to PEDSnet institutions have been increasing across all care settings and have increased at a greater percentage than visits overall, according to a comprehensive retrospective analysis. The largest proportion of SUVs among youth occur in the outpatient setting, and nicotine, cannabis and opioids are driving much of the growth. …
Between January 1, 2009 and December 30, 2024, there were 372,282 SUVs [mean age 16.1 (SD 2.23); 50.7% female] by 71,641 individuals. 54.1% of visits occurred in outpatient settings, 29.4% in the emergency department (ED), and 16.5% resulted in inpatient hospitalizations. SUVs increased in all settings over time. Further, since 2009, SUVs have increased by over 450% whereas all visits for this age have increased by less than 200%. Overall, seasonality trends remain unclear. However, when stratified by setting, there is a peak of visits to the ED in mid-February and mid-September. Nicotine was the most common substance (37.1%), followed by cannabis (31.9%), and opioids (15.1%). Nicotine, cannabis and opioids increased consistently in frequency across all care settings whereas alcohol-related visits have declined.
[emphasis added]
There’s another important question to address, that of whether young persons, “Gen Z”, comprised of individuals now between the ages of 14 and 29, are less likely to and are not engaging in high-risk or illicit opioid use at levels of incidence as great as their parents, or older cohorts have, contributing to the overall decreases in opioid overdose deaths, because they have been “scared straight”, “after witnessing devastation among other household members” per our opioid crisis experts.
We just dispensed with the first part of that question, invalidated the conjecture of their “not initiating opioid use”, by noting the lack of evidence for any such change and noting evidence pointing to the opposite conclusion.
What do we know about adverse childhood experiences and their effects on the mental health, capacity for emotional regulation, risk of and vulnerability to problem substance use, other high-risk behaviors, academic success, functioning and other forms of unwellness?
We know a lot, and it’s been established for decades.
Here’s one version of the common ACE survey now widely used in behavioral health and other healthcare settings.
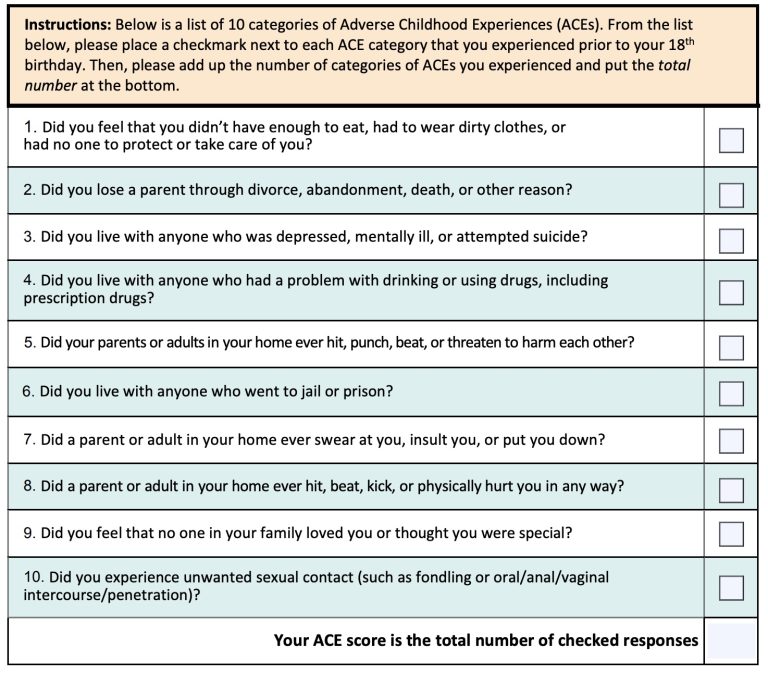
Now imagine the types of households and circumstances we are considering for the children potentially affected.
Right.
Let’s explore some of what is established about those effects and how they would impact, predictably, the kids who are experiencing them.
From a 2019 summary of research from the Johns Hopkins Bloomberg School of Public Health:

The opioid epidemic’s toll is wide-ranging and long-lasting, measured not only by lives lost but by families disrupted and communities strained. One dimension of the epidemic’s ripple effect that is critically important but not well understood is its impact on children. While there have been some dramatic and heart-wrenching media accounts of the struggles experienced by children of parents with opioid addiction—from foster care entry to disrupted learning to opioid withdrawal—essential questions remain: How many children are facing the consequences of the opioid epidemic? In what ways are they affected? And what is the societal cost? …
By 2030, the cumulative, lifetime cost of the “ripple effect” will be $400 billion. This includes additional spending in health care, special education, child welfare, and criminal justice stemming from the multiple impacts of parental opioid use disorder on a child’s physical, mental, and social-emotional health. It does not include productivity losses or missed opportunities.
These numbers should make every policymaker sit up and take note. Childhood adversity—such as living in a household with a family member with substance use disorder or being separated from a parent—has been strongly linked to a wide range of negative outcomes. These include poor school performance, early emergence of chronic disease, and an increased likelihood of developing a substance use disorder (the latter of which contributes to intergenerational cycles of addiction).
[emphsis added]
Also from 2019, from an informational, public service blog post from the North Carolina Institute of Medicine (NCIOM):

Opiate use is increasingly affecting children and families in North Carolina, and many stakeholders agree that primary prevention of trauma and adverse childhood experiences (ACEs), and the expanded infusion of trauma-informed practices into state efforts to address opiate use, are necessary tools for combating this problem.
Research has shown a link between trauma and ACEs and opioid addiction; while an estimated 75% of individuals with substance use disorders have experienced trauma, rates are even higher for individuals seeking treatment for opioid addiction. A 2016 study showed that people reporting five or more ACEs were three times more likely to misuse prescription opiates, and five times more likely to use injected drugs.[1] Strategies that focus on resiliency for children experiencing ACEs can help mitigate their impact and can help fight the opioid crisis facing our state.
Several states have initiated programs that focus on the prevention of childhood trauma as a key tool in addressing opiate use. In West Virginia, the Martinsburg Initiative aims to reduce opiate use by establishing community partnerships between schools, police, and other stakeholders. Participating stakeholders work to reduce trauma and ACEs through parenting classes, mentoring programs, mental health care, and other activities.[2] Generally, programs aimed at reducing childhood trauma and improving children’s well-being and mental health show significant cost savings; RAND estimates lifetime net benefits per child served at between $1,400 and $240,000, with the largest benefits associated with programs with longer-term follow up.[3]
[emphasis added]
This 2025 commentary in the Indiana Capital Chronicle lays out the scope of the problem and important aspects of ACE effects.
In 2017, more than 2.2 million children were identified as having a parent navigating opioid use disorder. In Indiana, that included more than 57,500 K-12 students. Indiana ranked 13th in the country per capita with 35 of every 1,000 K-12 aged students that had opioid affected parents.
These children are not addicts themselves, but have had a parent who misused opioids, was incarcerated for opioid use, or died due to an opioid overdose. Their parent’s addiction to opioids has left this population of students to be raised by a sober single parent, a grandparent, the foster care system, or some other form of kinship.
Essentially, our state lost a notable portion of the parenting population to the opioid crisis.
This parenting void has left their children, their families, the schools, and their communities struggling to cope with the aftermath. The children of addicts are overwhelming schools with higher rates of special education and behavioral health needs, the welfare service system, the health care system, the justice system, and Medicaid. They experience higher rates of abuse and neglect than children who do not have a parent with addiction issues and are at an increased danger of not graduating high school.
Specifically, children of addicts have lower rates of attendance and academic achievement, while also experiencing higher rates of behavior issues. …
While schools in Indiana scramble to navigate dwindling budgets, chronic absenteeism, excruciating incidents of escalating behaviors, and lagging academic achievement, the lion share of the very dollars that could help them were not even spent in 2023 and 2024.
[emhasis added]
We should be connecting some dots, including the “chronic absenteeism” associated with ACE within households of opioid-affected parents – with established increased risk of initiating opioid abuse – and the failure of expert-relied-upon invalidated in-school surveys to accurately measure youth opioid abuse trends.
And what about all those opioid household-generated foster care system placements? This recent, large study found that – no surprises – drug overdoses are more common.
More specifically, fentanyl use was not included in the analysis, grossly underestimating the scale of initiation of opioid use, and yet …
Foster youth had by far the highest rate of non-fatal overdose: 1.03%. …
Among unintentional overdoses, cannabis, benzodiazepines, opioids and stimulants were the most common. Unintentional cannabis and opioid overdoses also both increased in the years leading up to the pandemic in 2020.

As reported for places like West Virginia, front-line workers and researchers helping ACE-affected kids in foster placements don’t need to have dots connected, they see clearly what is plain to see, including researcher Erin Winstanley.
“If we want to stop intergenerational substance use disorders and this exposure to trauma, then we need to address the mental health needs of these kids, because we are predisposing a new generation to trauma,” Winstanley told MindSite News. Living in a home where a family member has a substance use disorder is considered an adverse childhood experience, and can lead to future drug and alcohol use, emotional problems and health and mental health disorders. “Protecting these kids is critically important,” Winstanley said.
[emphasis added]
Protecting them requires that they be seen, not hidden and betrayed.






