FAILED OPIOID CRISIS CURE SUBLOCADE: MORE LETHAL MISINFORMATION IN AMERICA’S TOP MEDICAL JOURNAL
Flaws in design and interpretation invalidate any conclusions of benefit from the injectable 30-day buprenorphine, consistent with other study outcomes and evidence
by Clark Miller
Published May 8, 2026
Here we have for our consideration another valuable and highly illustrative example – this one in America’s top medical journal – of a vetted (peer-reviewed) and published research study with fundamental, obvious flaws in design, interpretations, and validity (internal and external) that nullify the desperately needed conclusions.
Valuable not least of all as an imagined or real exercise or assignment for, say, graduate students in any health-related or research-focused program to develop competence in identifying gross errors that under any reasonable standards and circumstances would relegate the piece as unpublishable to protect the public from harm.
Those desperately needed conclusions were a force powerful enough to expose the fundamental flaw of relying on “post hoc” analyses to attempt to undo the original outcome of no finding of benefit from the gold-standard expert medical opioid cure as determined by the original design and planned statistical analyses of outcomes.
In plain language, the unspoken rationalization for the post hoc analyses (an illegitimate practice of reworking the data sets, outcome measures, and/or other aspects of the original design) to re-test for statistical significance was in order to achieve the results that must be achieved, to, in the repressed consciousness of the researchers, pharmaceutical sponsors of the research, peer reviewers, and journal editors, arrive at the conclusions of medical benefit that we have known must be true before the study was ever conducted.
That important mission was increasingly “desperate” in the context of prior studies of the potential benefit of sublocade pointing to harm rather than benefit, with high-risk opioid users continuing to engage in high-risk illicit opioid use while under the medical care provided by the 30-day injections. And desperate in the context of states and locales where Sublocade treatment has been broadly implemented evidencing no gain in reduced opioid-related deaths.

And desperately needed, those manufactured conclusions, in the aftermath of this $344 million NIH study to “test” the effectiveness of “proven”, “gold-standard” medical cures, including buprenorphine (active ingredient in Sublocade), which has been increasingly dispensed to diseased brains over decades of the worsening opioid crisis. Proven, gold-standard cures that have been, by expert and media consensus, already established as successfully treating the opioid crisis over past decades. Think about that.
Predictably, that largest ever NIH study failed to detect any benefit from medical cure buprenorphine, instead reaffirmed the established role of medication assisted treatment (MAT) in fueling the crisis. That’s awkward. With a price tag of $344 million in public healthcare funds.
That left only one option – post hoc analyses, which, it turns out, only re-reaffirmed the lethal role of medical cures in the crisis.
Attempts at damage control included researchers and top experts generating helpfully media-conveyed rationalizations, i.e., transparent lies, for the absence of their predicted and desperately needed results of any benefits from medical treatments to high-risk opioid users compared to “control” communities in which those treatments were not expanded, the rationalization that study communities were continuing to experience “headwinds” due to COVID effects.
That rationalization was nullified by the fact that the communities assigned to control versus treatment were, in fact, randomized, precluding any differential effects due to COVID.
That introduces some background, context, and one fatal, invalidating flaw for our current study of interest.
Here’s how MEDPAGE TODAY heralded the outcomes of that study.
That sounds quite promising, doesn’t it?
Another “game changer” in progress against the opioid crisis.
Let’s take a further look.
Let’s continue by considering the fact that subjects were paid a cash stipend per visit, as well as having all treatment costs paid, including transportation. Those visits would have included once weekly, with weekly urine drug screens (UDS) provided, through week 14, then monthly visits for injections and UDS through week 38, 6 additional visits, with plans for an additional 4 random UDS over that period.
As the researchers discreetly described it, “In addition, this study provided treatment at no cost, travel reimbursement, and stipends, which differs from clinical practice and may have affected retention.”
Readers here are familiar with the concept of cash payments for enticement to access a course of Sublocade injections, from our consideration of a program in Philadelphia, Prevention Point.
From that post –
The picture for Sublocade seems to be shifting, doesn’t it?
The more information we consider about it, its use, and claims made for it?
Good thing there’s this news piece from Philadelphia, in which we gain some significant details about the Sublocade experience, its medical provision, and some clarity.

At Prevention Point Philadelphia, officials report that interest in long-acting medications for opioid use disorder is growing significantly. The organization administered 312 Sublocade injections in fiscal year 2023 and double the number in fiscal year 2024.

Sublocade got approval from the U.S. Food and Drug Administration in 2017. While it’s been around for several years, Prevention Point clinic Dr. Serge-Emile Simpson said there have been challenges to prescribing it in the past.
It has a higher price tag compared to some other medications for opioid use disorder, so getting insurance to cover it was a problem. There was also special training required for providers who wished to administer the drug, Simpson said, and maintaining a local supply of the drug often came with other delays.
Now, more insurance plans cover Sublocade, and Prevention Point has a standing order with a local pharmacy to make sure the medication is readily available.
But there was still another hurdle to overcome, Simpson said. Providers noticed that some people in Kensington sell portions of their Suboxone prescriptions, a daily oral buprenorphine medication that comes in dissolvable strips, out on the street.
The people selling the medication would then use the money to buy food, clothes, bus tickets or even street drugs, while people buying the Suboxone would use it to manage withdrawal symptoms between injections or hits, or to supplement their own Suboxone treatment if they felt like their dosing wasn’t high enough to feel well, Simpson said.
“We could not get people interested in Sublocade because it would have bitten into their cash flow if they were selling some or all of their Suboxone,” he said. “That’s a significant sort of impediment to getting them started.”
That’s one way of describing the situation. Here’s another, from a previous post, outlining the central roles – as commodity, consumable, currency, other roles – buprenorphine has played in facilitating and fueling illicit economies of street opioid and other high-risk drug use.
From that previous post –
Back to our current post, and let’s digest that news from Philadelphia, to make sure it’s clearly understood.
The high-risk opioid users whom Prevention Point enticed to begin a course of Sublocade had to be paid, and paid cash, not vouchers, because they had been using their other buprenorphine formulation (Suboxone) on the streets to trade for illicit opioids, perhaps the most common and well-established use for “bupe” on the streets.
That doesn’t work, of course, for Sublocade once injected, so, naturally, predictably, it was required to provide them cash payments to gain their involvement in Sublocade injections, which, as we have seen, is clearly not a barrier to the continued use of illicit opioids to gain the effects desired by high-risk users.
So, another fatal flaw for the study, invalidating already invalid conclusions – we have no evaluation of what beneficial and protective outcomes due to 38 weeks of Sublocade “treatment” would have persisted past the end of treatment at 38 weeks and past the potentially primary motivator of regular, free transportation to a study site to pick up a cash payment.
“But!”, some may object, the outcomes for “opioid abstinence” rose quickly at the start of treatment and remained above 20 percent through the study.
Uh-huh, right, that appears to be so from Figure 2A, in which “missing” scheduled or random UDS are counted as a positive UDS for illicit opioid use.
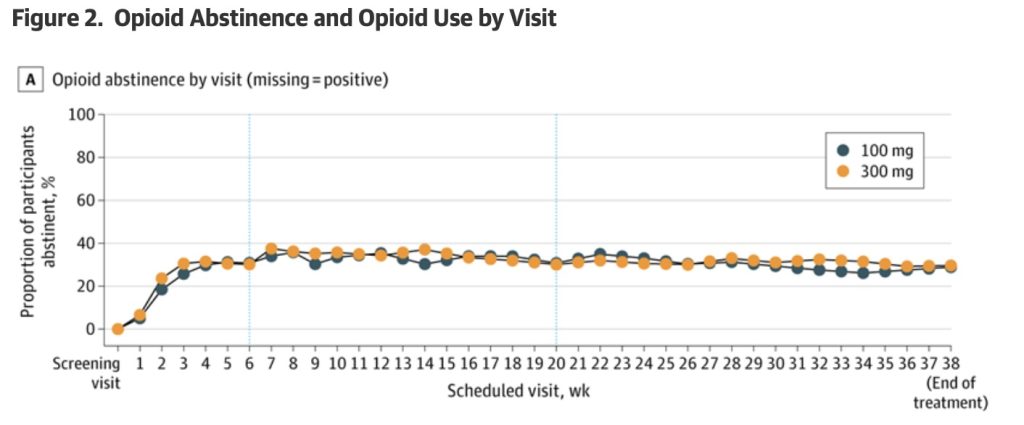
What we know is that “cheats”, or methods and strategies for defeating positive urine drug screens, are widely known and easily available.
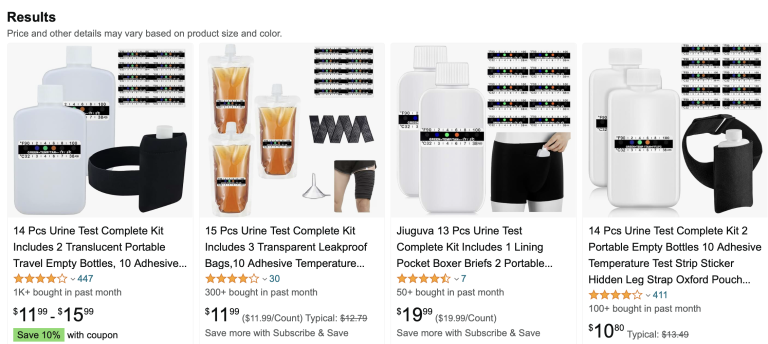
Under the circumstances of this study, defeating planned or random urine drug screens would have involved storing frozen quantities of one’s own urine after starting Sublocade injections and following a period of weeks without illicit opioid use, then using that “clean” urine from a device held at body temperature for the UDS.
Figures 2C and D represent the self-reports from subjects of the number of times opioids were used by them per week and the number of days per week opioids were used.
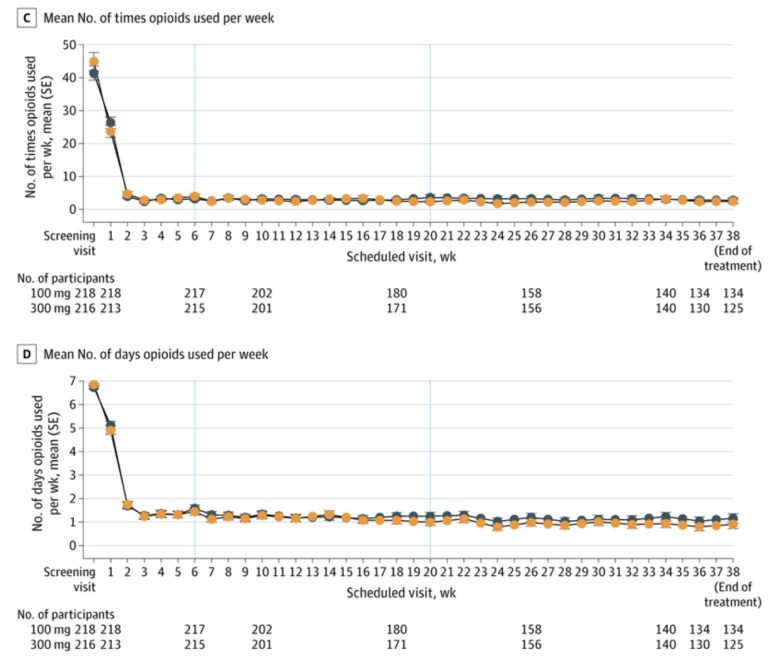
Those numbers seem remarkably low and remarkably consistent. We know, from studies of the reliability of self-reports in substance use research, that they are not valid.
They are not supported by the UDS results, which are not valid unless the act of urination was observed for each UDS.
For the UDS protocols used in this study, Fentanyl use would have become undetectable in as little as 4 days, over the period of 6 months of monthly UDS, with 4 additional random UDS.
The study population members were engaged in treatment programs at a variety of facilities and locations and described as “treatment seeking”. We do not know to what extent they may have been mandated or otherwise at risk of serious to grave consequences for positive UDS related to their individual programs and circumstances.
In short, we are not able to have confidence in the outcomes for abstinence or frequency of illicit opioid use over the study period.
We are even less able to evaluate their frequency of nonfatal overdose over the study period, given the shift in North America, over recent years and over increasingly successful naloxone campaigns, of overdose reversals shifting to predominantly performed by peers, family members, passersby, or laypersons, and which are not reported.
There are, of course, often large disincentives for the reporting of nonfatal overdoses by high-risk opioid users in and out of treatment.
In short, the study does not support conclusions that Sublocade provided benefit to subjects related to their compulsive, high-risk use of illicit opioids.
And with no post-treatment follow-up, we have no way to evaluate the effect of providing regular cash payments on aspects of motivation, retention, veracity of self-reports, and validity of UDS.
Given those invalidating elements that include lack of external validity, along with consistent outcomes of no benefit or continued high-risk opioid use in prior studies, it is fortunate that we also have available a large, “natural experiment” spanning years of enhanced provision of Sublocade in real treatment settings, in the Canadian province of Alberta.
From that post –
That brings us to a point at which some explanations are demanded, and explanations owed to Albertians, Canadians and Americans, to anyone who has trusted in the public health experts, institutions and media to provide truth and competent guidance to address the lethal crisis worsening over decades.
Because in Alberta, the persistently worsening crisis, moderated only by desperate, intensive naloxone campaigns to reduce the death count from increasing high-risk opioid use, has occurred over years of gold standard “treatment” expansion investment of $200 million, in a province of about 5 million Canadians.
And because the focus of that $200 M investment was provision of the “game-changing” proven, expert opioid cure Sublocade, an injectable, 30-day formulation of buprenorphine that cannot be diverted or used, like other “bupe” formulations, as street currency for fentanyl.
That investment in provision of the gold standard, injectable medical opioid cure began in 2021.

The Alberta government announced Wednesday it will fully cover the cost of the injectable opioid treatment drug Sublocade.
As opposed to tablet versions, the injectable treatment lasts in a person’s system for 30 days and provides stabilization, reduces cravings and provides enhanced protection against overdose, the province said.
“There is hope for people with addiction,” said Mike Ellis, associate minister of mental health and addictions. “Recovery is possible.”
“This option will save lives,” Ellis said.
“The addition of Sublocade to the publicly funded formulary and removal from special access will significantly reduce barriers to this medication. Recovery-oriented care is about providing options to Albertans with addiction and this option will save lives and support recovery,” Ellis added
Having the costs of Sublocade covered “will be a game-changer for addiction treatment in Alberta,” said Dr. Monty Ghosh, president of the Alberta Medical Association.
“This will increase treatment options for individuals with opioid addiction. Addiction medicine physicians across Alberta will be grateful to have another tool to treat opioid addiction, especially for our various vulnerable clients who previously could not afford this life-saving medication.” …
“That option is important to have on the table for some people who have an opioid addiction disorder,” said Elaine Hyshka, assistant professor at the University of Alberta’s school of public health. “Cost should not be an impediment to access care.
[emphasis added]
That’s high praise – and from a consensus of experts! – for a “treatment” that was, predictably, bound to be evidenced as lethally failing.
Alberta went in full tilt for Sublocade.
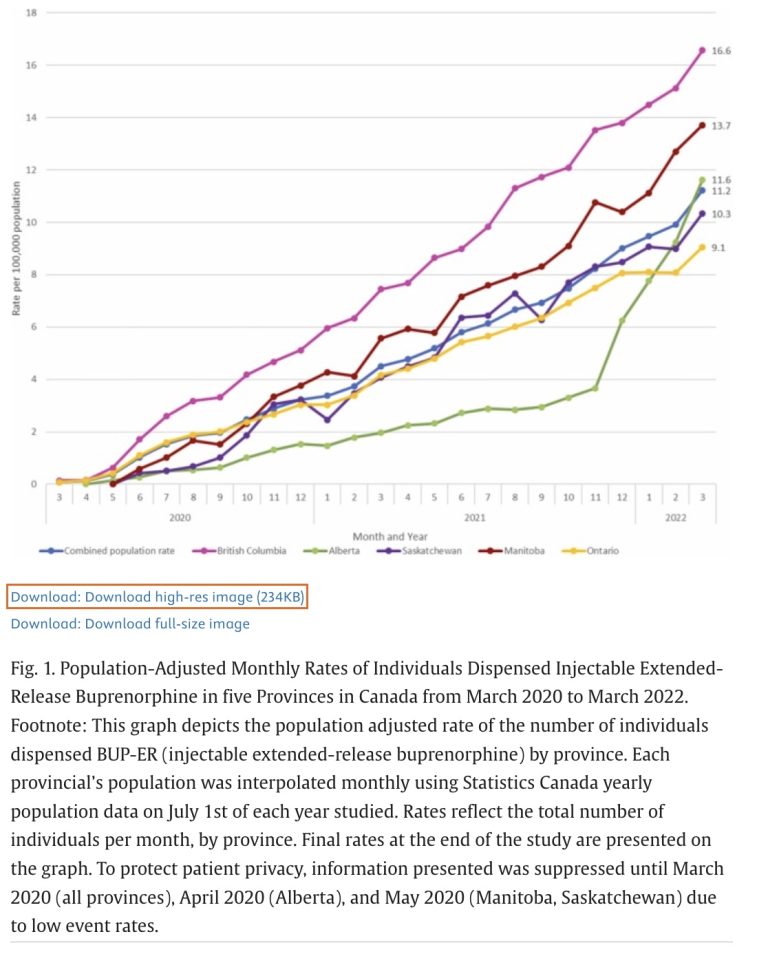
(Alberta data are represented by the green line in the first two figures below. )
Highlights
Extended-release buprenorphine (BUP-ER) is a novel form of treatment for opioid use disorder available in Canada since 2020.
Use of BUP-ER rose quickly across Canada since approval, but varied by province.
BUP-ER use is highest in rural regions, reflecting improved accessibility to treatment in some parts of Canada.
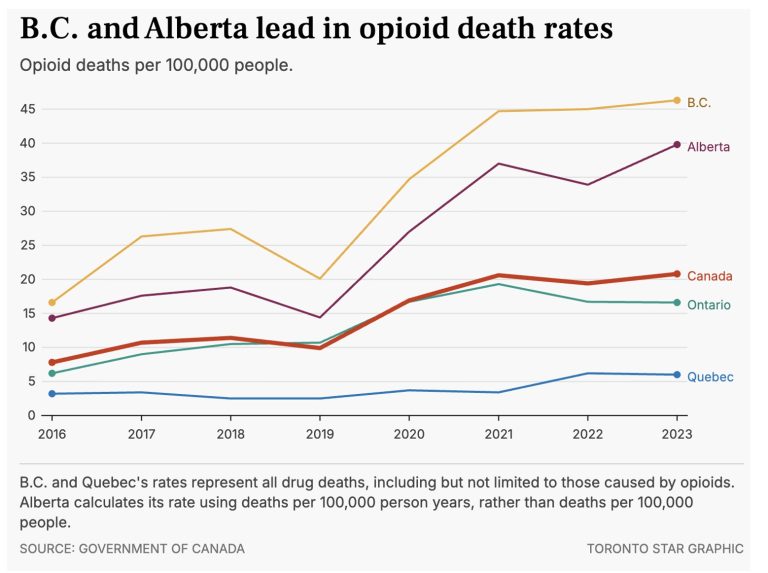
Here’s another line graph comparing Canadian provinces.
In this case, data illustrate how opioid overdose deaths surged in Alberta compared to other provinces during and immediately following the years over which the provision by medical providers of “game-changing” sublocade was surging.
From a 2021 report on Alberta’s treatment expansion –
“We’re building five new long-term drug addiction therapeutic treatment communities across the province, including partnerships with First Nations communities that have been hard hit by the opioid crisis.”
The province has put more than $200 million into initiatives to address the opioid crisis, the premier said.
And from this 2025 CBC report, traditional gold standard treatments for problem opioid use continued to expand per Nathaniel Dueck, press secretary for the Ministry of mental health and addiction –
“He said Alberta started accepting clients at three of its recovery communities starting in May 2023, with eight more being established as part of its response to the addiction crisis.
The province also said it added more than 10,000 publicly funded treatment spaces and removed daily user fees for residential treatment.”
Things just don’t add up.
Or do they?
Actually, things always add up,
just not in ways they are desperately needed to, but for anyone overcoming the cowardice that would otherwise inhibit and blind them from seeing and expressing the obvious.
Obvious, from decades of evidence, that:
There has never been strong, let alone compelling evidence (and here) that American Medicine’s gold standard cures for substance use provide benefit.
Or that substance use is a medical condition at all, treatable with medical interventions.
It turns out, as explained and established here in multiple posts, that precisely as in the avoidable – avoidable if not for the cowardice and gross incompetence of American Media – generation of the opioid crisis as we know it enabled by fabrications by America’s medical/research/media collusion, there has never, not ever, been a legitimate body of research evidence to confidently establish, let alone strongly support, the use of substitute opioids (bupe or methadone) as treatments or as beneficial for opioid dependence.
Instead, all lines of diverse evidence point to what should be obvious – the runaway dispensing of opioids that are routinely used with other, illicit opioids (methadone), and/or serve as consumable, commodity and currency in street economies of illicit high-risk opioid use (bupe) have in fact fueled the lethal epidemic.
The most potent ways in which the “miracle” doctor-dispensed pills and other magic potions predict failure is to instill in compulsive substance users the belief that passive interventions to adjust brain chemistry are “treatments”, are addressing a generic neurobiological block or deficit or disease of the brain that explains addiction, instead lethally instilling passivity, dependence and lies, and robbing compulsive substance users of the necessary factor established as central to stopping problem use, self-efficacy, the shift to belief in one’s own competence, autonomy, strength, and effective use of resources with inner psychological change to do away with the compulsion to escape distressing inner states by use of chemicals.
Some lies must be desperately protected, no matter the cost.
Related upcoming post, with more from America’s top medical journal –
NEW RESEARCH REAFFIRMS PREDICTED LETHALITY OF MEDICAID EXPANSION OF ACCESS TO OPIOID CRISIS MEDICAL CURE BUPRENORPHINE






