NEW RESEARCH REAFFIRMS PREDICTED LETHALITY OF MEDICAID EXPANSION OF ACCESS TO OPIOID CRISIS MEDICAL CURE BUPRENORPHINE
States selected based on larger Medicaid-fueled gains in buprenorphine (Suboxone) medical dispensing had worse opioid overdose outcomes than other states over the period of expansion, predictably. We know why.
by Clark Miller
Published June 5 , 2026
Following the clear outcomes of lethal effects for the medical opioid crisis cure buprenorphine in a $344 million NIH (National Institutes of Health) study intended to establish benefit for that substitute opioid increasingly dispensed as the proven gold standard cure over decades of the worsening crisis, the new study in America’s top medical journal is another desperate attempt to generate positive outcomes by pre-selection of the study population. In this case, that was by arbitrarily selecting states beginning expansion after 2018, to demonstrate larger increases.
As reported here on the research appearing in the Journal of the American Medical Association (JAMA) –
In the eight states that expanded Medicaid after 2018, the number of people receiving prescriptions for the opioid addiction treatment medication buprenorphine increased dramatically, according to a paper that researchers will present next month.
The states that expanded Medicaid before that period also saw gains, but they were generally smaller. That’s because other changes, aside from Medicaid expansion, made buprenorphine easier to get after 2018.
The researchers found that among all patients — those covered by Medicaid, other insurers and the uninsured — the number of buprenorphine prescriptions increased in the eight most recent Medicaid expansion states (Idaho, Maine, Missouri, North Carolina, Oklahoma, South Dakota, Utah and Virginia) by more than 21% between 2019 and 2023. Maine, Oklahoma and Virginia saw the most dramatic increases.
Among the states that expanded Medicaid in 2018 or before, Kentucky, Vermont and West Virginia experienced the largest boosts. The study, published in February in JAMA Network Open, was conducted by researchers from Rutgers University and Indiana University, based on pharmacy claims data from retailers across the country.
Here’s the original research title, in JAMA,
Here are the “Conclusions and Relevance” from that Original Investigation in America’s top medical journal.
Conclusions and Relevance In this cross-sectional study using contemporary data and methods, post-2018 Medicaid expansions were associated with substantial increases in buprenorphine treatment, particularly in high-need states operating under newer prescribing regulations. These findings underscore Medicaid expansion’s role in improving opioid use disorder treatment access and can inform state and federal efforts to expand evidence-based care.
Clearly, these are positive and encouraging outcomes. That goes without saying.
As the experts conveyed to us,
“These findings underscore Medicaid expansion’s role in improving opioid use disorder treatment access and can inform state and federal efforts to expand evidence-based care.”
Who could question that?
There’s really nothing to add.
Except … I mean … what if … I mean … so … should we wonder how things went in those states? … for those enrollees? … how they did? Of course, we know that they would have benefited from the proven, gold-standard expert treatment, the medical cure for problem opioid use. There can be no doubt, that’s why it’s so important to pay attention to experts trying to help us understand why these types of findings are so important … so important in their provision of evidence-based care to high-risk opioid users.
Okay, so it can’t hurt, can it? To take a look at the actual outcomes for measures of opioid crisis severity and course in those states that gained so much, relative to others, in provision of the evidence-based medical cures?
We could do that just to reinforce the results and their conclusions, right?
Let’s take a look.
Let’s remind ourselves, to help us track through what we want to explore, that the 8 states are:
Maine, Virginia, and North Carolina
Missouri and Oklahoma
South Dakota, Utah, and Idaho
The three identified as having the greatest gains in enrolling Medicaid patients into services in which they are provided, by prescription, the common street currency for fentanyl, aka “burenorphine”, are Maine, Oklahoma, and Virginia.
Let’s start with this graphic from a 2026 KFF report. Markings are added to indicate states of interest.
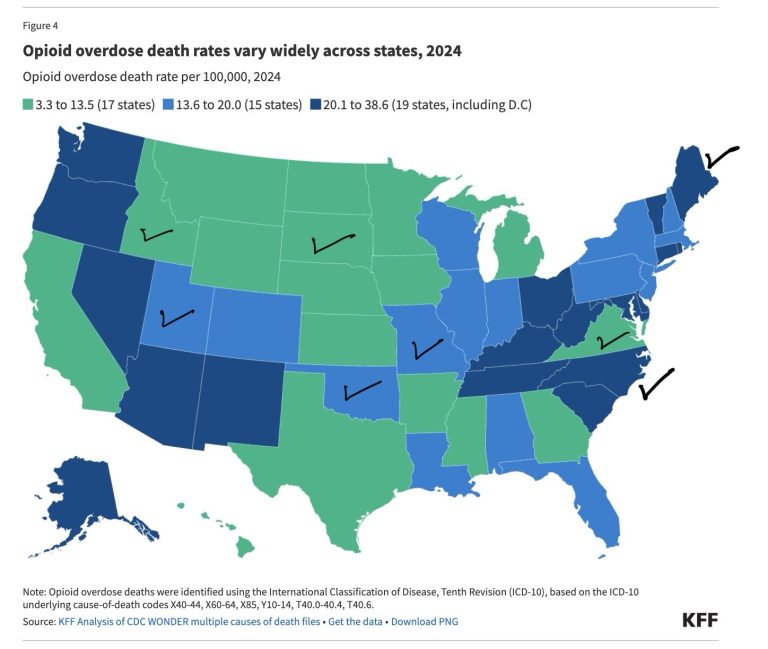
It’s important to recognize that while illustrative in some ways, the graphical representation is not relying on continuously variable values for comparison, instead ranks, or groupings, into three levels of opioid OD death rates (per 100,000) arbitrarily defined as represented. That necessarily entails imprecision in interpretations and validity. Our Medicaid expansion state Virginia, for example, from the interactive graphic, has a value of 13.3 deaths per 100k for 2024, and if, by imprecision or other errors, the actual estimated value should have been 13.6, that would have placed Virginia in the middle group for fatal overdoses, significantly affecting potential reasonable conclusions.
Working with what is presented, several points seem notable, following 6 years of expanded Medicaid provision of prescribing of buprenorphine:
– Two of the 8 expansion states are in the group of states with highest rates of overdose deaths.
– One of those, Maine, was identified as among the 3 of those 8 states with largest expansion of medical provision of substitute opioids to high-risk opioid users.
– The group (green) of states with lowest overdose rates includes 3 of the 8 expansion states, 37 percent of the expansion state group), and includes 38 percent of remaining states (42 states), that is, expansion states were not disproportionately more likely to be in the group of lowest opioid overdose rates.
Let’s look at another graphic from the same report that does use continuously variable values, thus allowing more precise and valid impressions.
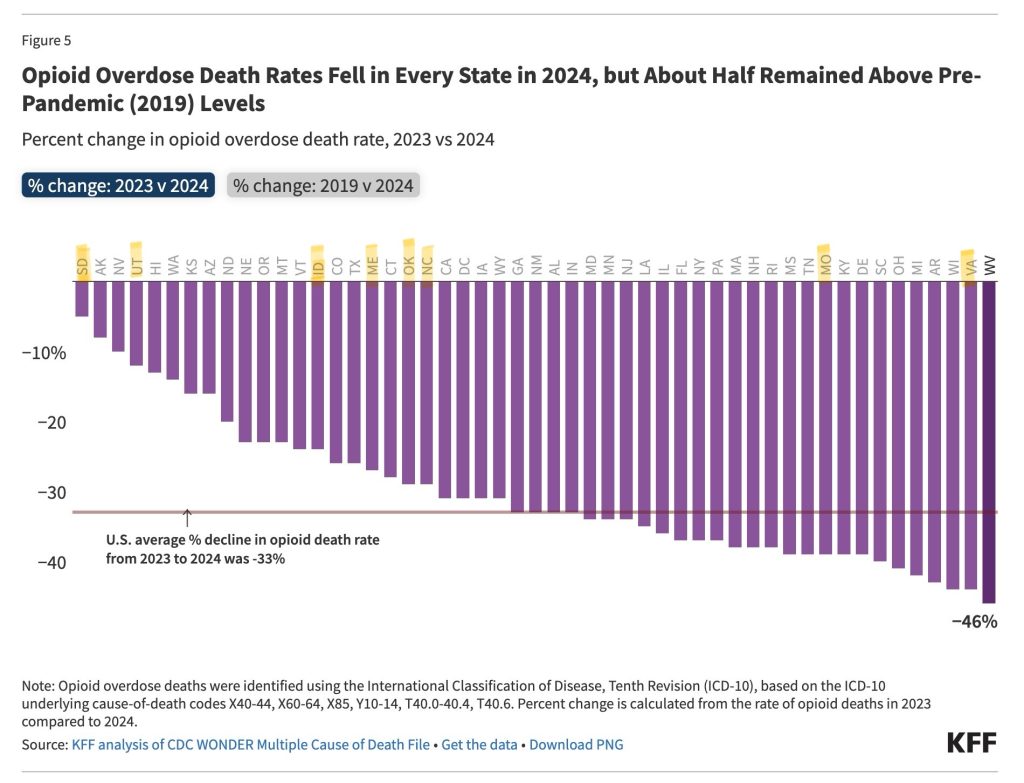
Six of the eight states with increased provision of medical opioid dependence cure buprenorphine via Medicaid expansion were below the average for all states. From the interactive graphic, the average percent decrease for the 8 states was -26% compared to -33% for all states. On the presumption of benefit in reduction of high-risk opioid use, thereby of overdose, and thereby of opioid overdose deaths, from enhanced provision of gold standard cure buprenorphine, that average decrease should have been higher for the 8 expansion states.
Virginia, one of two of the 8 expansion states above the average, is an apparent outlier that we will come back to.
A separately reported graphic here allows us to consider, for the 8 expansion states compared to other states, outcomes for percent increase in deaths due to fentanyl and “other synthetic opioids” over 2023 compared to 2022.
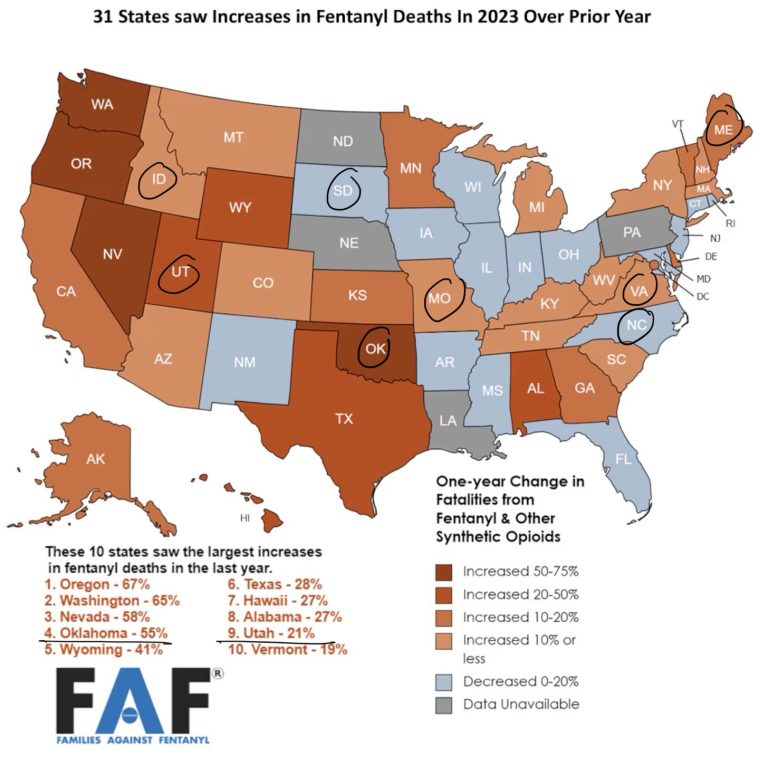
This graphic nearly speaks for itself, but not quite.
Two of the 8 Medicaid expansion states in the JAMA research article we are considering were in the ten states of all states for greatest increases in deaths due to fentanyl deaths in 2023, after 5 years of presumed benefit from increased medical provision of opioid cure bupe. One of those is Oklahoma, in the top three of the 8 states for increased dispensing of Buprenorphine. Another of those top 3, Maine, was 14th highest in increase in fentanyl deaths, reported here.
Considering the other 42 states, 62 percent had increases in such deaths, and among the study states, 75 percent did.
Of the 42 non-study, non-expansion states, one-third had decreases in such deaths, and among the study expansion states, 25 percent did, South Dakota and North Carolina.
And that’s where it becomes important to take a closer look.
Let’s do that.
The graphic above represents South Dakota as achieving a decrease in opioid OD deaths in 2023 compared to 2022. But that’s not what the state dashboard presents, which is opioid deaths steadily increasing over 5 years from 2019 – the beginning of Medicaid expansion fueling increased medical cure provision – through 2023, then dropping in 2024.
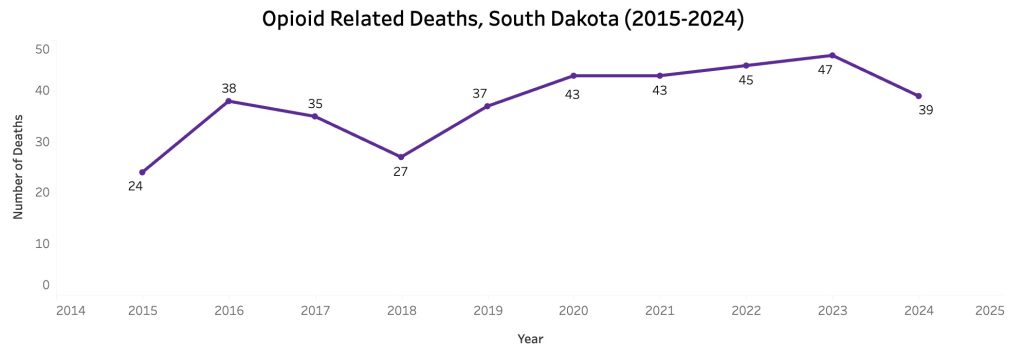
That drop corresponds to a significant increase in distribution of naloxone in South Dakota, by about 35 percent in 2023 and continuing into 2024, compared to prior years 2022 and 2021.

More importantly, as described in this May 2025 post, until July of 2023, laypersons in South Dakota could not legally purchase or carry naloxone to use to reverse a potentially fatal opioid overdose. Yes, that’s right, from that post –
“Why Wait?” one headline seemed to scream, the news piece describing legislative changes required so that, not until July of 2023, bystanders could obtain and carry the opioid fatal overdose reversing drug.
No, really. July, 2023.
Bystanders who witness an opioid overdose in a public space, restaurant or workplace only have one option under existing state law: call 911 and wait for help to arrive.
But waiting puts lives at risk, said Rep. Brian Mulder, R-Sioux Falls.
Under current law, medications used to treat opioid overdoses in emergency situations — such as naloxone, often delivered as Narcan nasal spray — are only able to be purchased and carried by first responders, nurses and people who know someone at risk of overdose.
That will change on July 1.
Back to our current post.
And to summarize for South Dakota.
In mid-July of 2023, laypersons, increasingly involved due to proximity (when every second counts), have been predominantly responsible for opioid overdose reversals nationwide, accounting for all drops in opioid overdose deaths (see, for example, here). In South Dakota, that lethally late change in allowance of laypersons to carry and use naloxone corresponds closely, along with increased provision of Narcan units, to the decreases in OD deaths beginning in 2024.
Prior to that and over 5 years of increasing provision of medical opioid cure buprenorphine under Medicaid expansion, opioid OD deaths increased.
Let’s move on.
To North Carolina, one of the 2 late Medicaid expansion states in the study and, like South Dakota, represented as having a decrease in fentanyl deaths in 2023 compared to 2022. But in 2024, North Carolina remained among the 16 or 17 states with the highest per capita opioid death rates.
Described and illustrated in this post, it’s the same story – OD deaths rising steadily through the years of Medicaid expansion of medical opioid cure, then dropping suddenly beginning late 2023, corresponding to dramatic increases in distribution, training, and use of naloxone to prevent the deaths, the numbers of estimated saves many times greater than needed to account for the magnitude of reduced deaths.
What about Virginia?
As described in this post, it’s the same story.
Opioid high-risk use, overdose, and fatal overdoses continued to increase over those years of Medicaid-fueled expansion of doctor-dispensed substitute opioids, until – and not until – dramatic, intensified, targeted naloxone campaigns reversed that iatrogenic harm, and deaths began to drop.
Let’s remind ourselves of how America’s healthcare experts conveyed to us, in America’s top medical journal, the relevance of their findings for the role of Medicaid expansion in addressing the worsening opioid crisis.
“These findings underscore Medicaid expansion’s role in improving opioid use disorder treatment access and can inform state and federal efforts to expand evidence-based care.”
Who could question that?
We just did, and found it to be a lethal lie.
And we’ve known that all along, because it’s been evident and predictable. It’s what we can expect from America’s compromised, impaired expert class.
As related to Medicaid expansion, revealed in this post from January of last year.
And more generally, from this April 2019 post outlining the profoundly diminished capacity for critical thought and veracity driving lethal epidemics, exposing the lethal cluelessness.
It’s always been there, always revealable, never exposed, protected at any cost.






