SAN FRANCISCO FENTANYL OVERDOSE DEATHS INCREASED LAST YEAR, PREDICTABLY
As elsewhere, naloxone saves can’t keep up with the magnitude of high-risk use and overdose driven by expert treatment failure
by Clark Miller
Published February 27, 2026
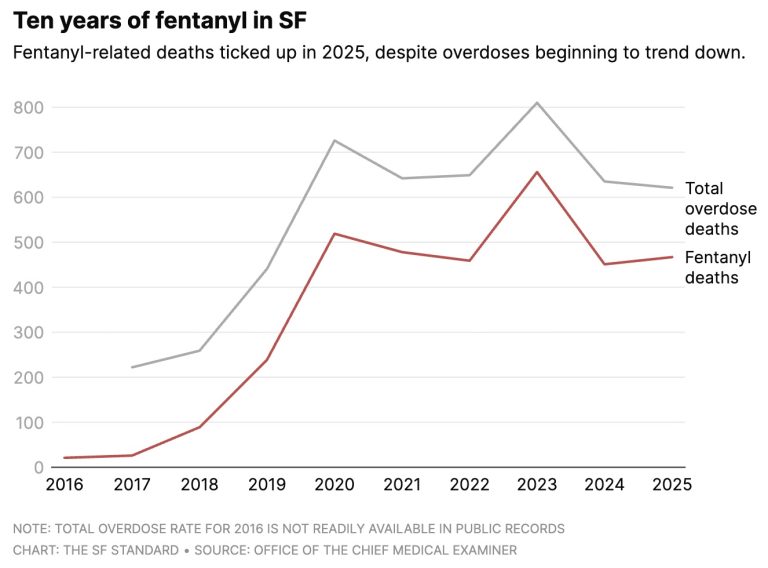
There are no surprises in the news from San Francisco, where fentanyl overdose deaths trended back up last year, after periods over which effective naloxone campaigns had more than compensated for the factors established as fueling and driving high-risk opioid use and deaths.
From a February 5, 2026 piece in The San Francisco Standard –

San Francisco’s expert strategy is the same that earned Baltimore its place as America’s opioid death capital – doubling and tripling down on medical dispensing of the abused, diverted, and in other ways centrally important opioids functioning in illicit opioid street economies of high-risk use. And deaths.
In San Francisco, launched in 2024, that took the form of SF Department of Public Health (DPH) workers out at night in city areas of high-risk opioid use, hooking up those users to quick, easy access to buprenorphine and methadone, as pictured above.
The buprenorphine could, once started, be provided by phone contact with prescribers.

A “Night Navigation street care team” walks the streets of the Tenderloin every night offering immediate drug addiction treatment to unhoused people addicted to fentanyl and other opioids, the health department said
The team can connect users in real-time with a doctor who can prescribe medication by telephone. From March to May, 440 people were put in touch with doctors, and 369 got prescriptions. About 40% of those prescriptions were filled.
Most received buprenorphine, which is as effective as methadone but more accessible, said Dr. Hillary Kunins, director of behavioral health services and mental health at the department.
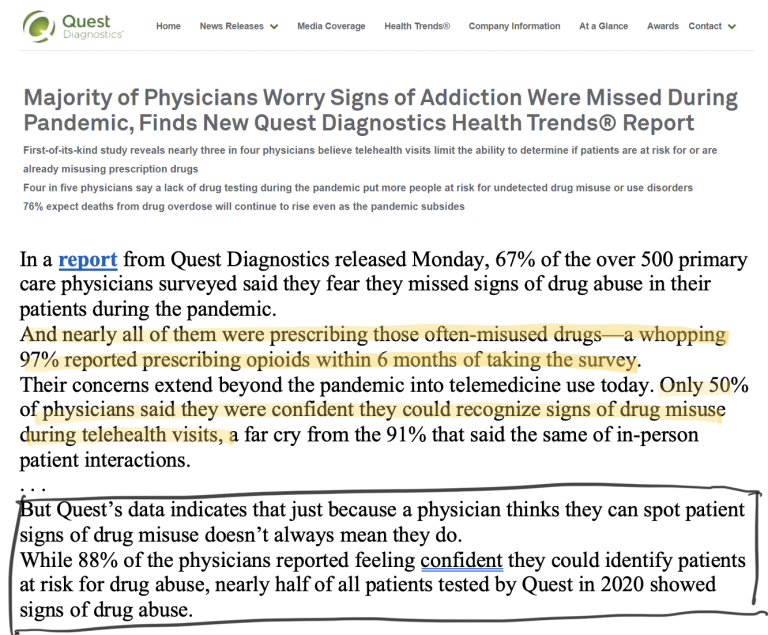
Here’s how surveyed medical prescribers responded regarding their use of telehealth to dispense “treatment” opioids once safety standards were dropped in response to COVID conditions –
Early in 2025, the signs were apparent, described in this SF follow-up post.
From that post –

“For people with opioid use disorder, including fentanyl addiction, the most effective medications are buprenorphine and methadone, each which reduce the risk of mortality by approximately 50%,” the agency said.”
Report of that predictable failure came as San Francisco also reported a return to increasing opioid use-related deaths –

“This doesn’t seem like it’s working the way we had hoped”
That’s not a good look for the experts, especially with evidence establishing that any and all previous reductions in opioid overdose deaths have been entirely attributable to intensive Narcan campaigns, the naloxone distribution acting as harm reduction to mitigate established roles of bupe and methadone in fueling the lethal epidemic.
An even worse look for public health and medical experts to somehow decide to implement distribution of the common street currency for fentanyl to high-risk opioid users, as if that might be helpful?
So it makes sense, at least, the medical expert comment that, “This doesn’t seem like it’s working the way we had hoped”.
Back to our current post.
“doesn’t seem like it’s working”
That’s one way to describe the crisis persistently worsening over decades of increasing provision of expert, gold standard cures.
Until the culpability and human costs of that weak, restrained, evasive use of protective language become intolerable and too exposed to hide.






