IT’S HARD TO HIDE A WORSENING OPIOID CRISIS
Even desperate, intensive, effective life-saving naloxone campaign overdose reversals, increasing by the thousands, cannot overcome lethal expert gold standard treatment failure
by Clark Miller
Published March 6, 2026
Three of the headlines appeared in a single internet search for news articles on a recent date (February 20), another 2 days later, with the search words “opioid crisis”.
They are the emerging signs of a worsening crisis that will be buried under the orchestrated onslaught of celebratory major media pieces noting reductions in opioid overdose deaths and soothingly, protectively mystifying what those shifts could possibly mean, to hide what they do mean.
And they will continue to emerge, generated by what is real, only because America’s maleficent, lethal media/expert collusion has not achieved full control.

According to the Montana Department of Health and Human Services, the number of drug samples testing positive for fentanyl was cut in half between 2024 and 2025.
A decrease that large likely means there is less fentanyl on Montana’s streets. But that didn’t equate to fewer overdoses.
Ambulance services responded to roughly 250 more suspected opioid overdoses in 2025. That’s a 35% increase compared to the previous year. Overdose deaths also ticked up slightly.
Agencies in Stanislaus County are alerting the public to an alarming increase in drug overdose and accidental poisoning deaths.
An advisory was released Thursday through the Opioid Safety Coalition and was posted on social media by agencies including the Stanislaus County District Attorney’s Office.
Stanislaus County averaged two to three fatal drug overdoses or poisonings per week in 2025, which was a decline when compared with previous years.
The rise in suspected drug-related deaths this week was higher than those recent trends, which prompted the notification, said Dr. Bernardo Mora, medical director of county Behavioral Health and Recovery Services.

In 2022, according to County data obtained by CBS 8, approximately two people were dying each day in San Diego County from fentanyl. There were 802 fentanyl-caused deaths that year in the County.
However, in 2025, the data reflect 340 deaths in San Diego County.
Dr. Nicole Esposito, San Diego County’s Chief Population Health Officer, said that even with a huge drop, the number of deaths is still slightly above pre-pandemic levels.
“Overdoses are still happening every day. I think that people are just, one, have naloxone and just know how to use it… It’s definitely a step in the right direction, but there’s still a lot of work to do,” Noah Chase, the overdose response trainer for “A New Path,” a non-profit organization contracted with San Diego County, said.
(emphasis added)
Each of the headlines and stories is revelatory of the worsening crisis, the last, from San Diego county, by what is hidden and how, as much as what is explored.
Let’s take a look.
The report from Montana highlights several critical distortions that have allowed deceptive messaging to hide the worsening crisis.
Both nonfatal and fatal opioid overdoses have increased there, per the report.
As explained in detail in many posts here and here, the decreases that have been occurring in fatal opioid overdoses are not a measure of an improving opioid crisis, instead of the opposite, because those decreases are established as accounted for by desperate, emergency, harm-reducing naloxone campaigns necessitated by the lethal failure of expert, gold standard “treatments” to reduce high-risk opioid use, which is increasing.
High-risk use increasing as in Montana, as evidenced by the surge in EMS (ambulance) response to overdoses = high-risk use. What we know, is established, is that those nonfatal opioid overdoses over past years, as measured by EMS response and/or ED (emergency department) records have increasingly become larger and larger undercounts, underestimating total opioid overdose (= high-risk use) levels.
Just as salient is the important meaning of those measures of a worsening crisis in Montana elevating, along with the report that,
“According to the Montana Department of Health and Human Services, the number of drug samples testing positive for fentanyl was cut in half between 2024 and 2025.
A decrease that large likely means there is less fentanyl on Montana’s streets. But that didn’t equate to fewer overdoses.”
Understanding the meaning of that observation is key to understanding why recent explanations for general, widespread opioid overdose reductions based on “supply shock” or fentanyl supply or quality disruptions are in fact baseless, are absurd on their face when we consider the behaviors of high-risk opioid users and other factors, including in the upcoming post, “THE LETHAL ROLE OF ABDICATION OF THOUGHT IN A WORSENING OPOID CRISIS”.
It may be worth keeping in mind the simple, incontrovertible fact: the only way that illicit opioid supply disruptions can have any effect in reducing opioid overdose deaths is by reducing opioid overdoses, which have not been decreasing.
From New Hampshire, as in Montana, the increases were in nonfatal as well as fatal ODs, thus a valid measure of increased high-risk use, that is, of a worsening crisis.
Additional material reported here includes that –
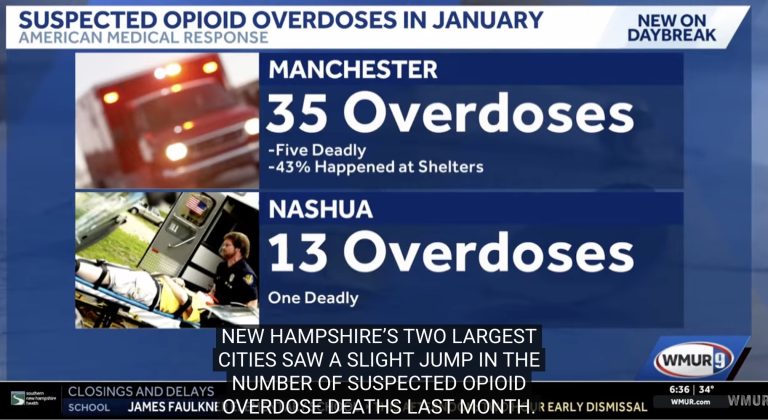
American Medical Response said medics responded to a total of 48 suspected overdoses in New Hampshire’s two largest cities in January.
According to AMR, 35 of those overdoses happened in Manchester, and 13 happened in Nashua. There were five suspected opioid overdose deaths in Manchester and one in Nashua.
The combined number of suspected overdoses was above the recent record lows but was still close to the rolling 12-month average, AMR said. The combined number of reported fatal overdoses was slightly higher than the 12-month average.
That is to say, in real speak, nonfatal and fatal opioid overdoses increased in New Hampshire’s two largest cities.
That news must have been jarring to state residents after this news headline from November of last year.
From the recent post deconstructing that “Good News” beginning with an excerpt from the NH JOURNAL story –
After nearly a decade of grim statistics, New Hampshire’s getting some very good news in the fight against opioid death and addiction.
The latest data show opioid deaths and overdoses have dropped dramatically, with overdose deaths and emergency responses falling to their lowest levels in a decade in the state’s two largest cities.
No one died from opioid-related overdoses in Nashua last month, and Manchester saw three overdose deaths, continuing a trend that health officials say could mark a genuine shift in the long-running epidemic.
“October suspected opioid ODs were well below recent averages and continue to trend in a very encouraging direction,” said Chris Stawasz, Northeast regional director of government affairs for Global Medical Response, Inc.
Stawasz, who began tracking opioid overdose statistics in Manchester and Nashua for a decade, said 2025 is shaping up to be the best year yet in the fight against opioids. AMR medics responded to just 35 suspected opioid overdoses in the two cities in October — 17 in Manchester and 18 in Nashua.
“The combined (two) city total of 35 was the lowest total number of suspected opioid ODs in one month since AMR began tracking them 10 years ago,” Stawasz said. “The 17 suspected opioid ODs in Manchester were by far the lowest one-month total since AMR began tracking them 10 years ago.”
[emphasis added]
THAT IS “GOOD NEWS” !
It is, isn’t it?
It would have to be, right?
Not just for reduction of opioid overdoses and fatal overdoses, but for “addiction” itself, it says, right in the article.
The expert and writer make it clear, don’t they, that when they refer to opioid “overdoses”, as opposed to “opioid overdose deaths”, they are referring to the number of opioid overdoses that were recorded when emergency responders were called and involved, that’s where they got their data, their numbers – from the incidents logged by emergency medical responders and that become part of a searchable, available record. That’s clear.
Oh … wait … that’s a problem, isn’t it? A really big problem that we’ve seen before.
Because what we know, what is established (and here, for example), is that over past years desperate, dramatically successful campaigns across the U.S. have placed potentially fatal overdose reversing naloxone into the hands of laypersons and others proximate to overdosers – where every second counts and naloxone saves have surged. And we know that along with that dramatic shift from emergency responders reversing potentially fatal ODs to increasingly community members, fewer and fewer potentially fatal opioid ODs are being formally reported or end up in the type of searchable databases that can be accessed for reports or news articles. AND, of course, that establishes that opioid overdoses (= high-risk opioid use = gold standard treatment failure) are being grossly undercounted.
Using those known underestimates of high-risk use and potentially fatal overdoses as evidence for gains against the opioid crisis, let alone against “addiction,” is what we would have to characterize most generously as the abject failure of America’s expert and media classes, more realistically as the distortions and mystifications necessary for them to attempt to escape culpability.
Back to our current post.
The increases in overdoses had to be explained away and were, here.
“AMR’s northeast regional director, Chris Stawasz, said, “Due to the nature of the opioid epidemic and its clear history of unpredictability, it is always possible that the trend of lower numbers could quickly change. Overall, the trend continues in the right direction.”
A worsening epidemic by all valid measures is not “the right direction”.
Thought-free media subservience to the needs of America’s lethal expert/medical/public health collusion is a potent factor in the worsening crisis, messaging medical misinformation that is lethal.
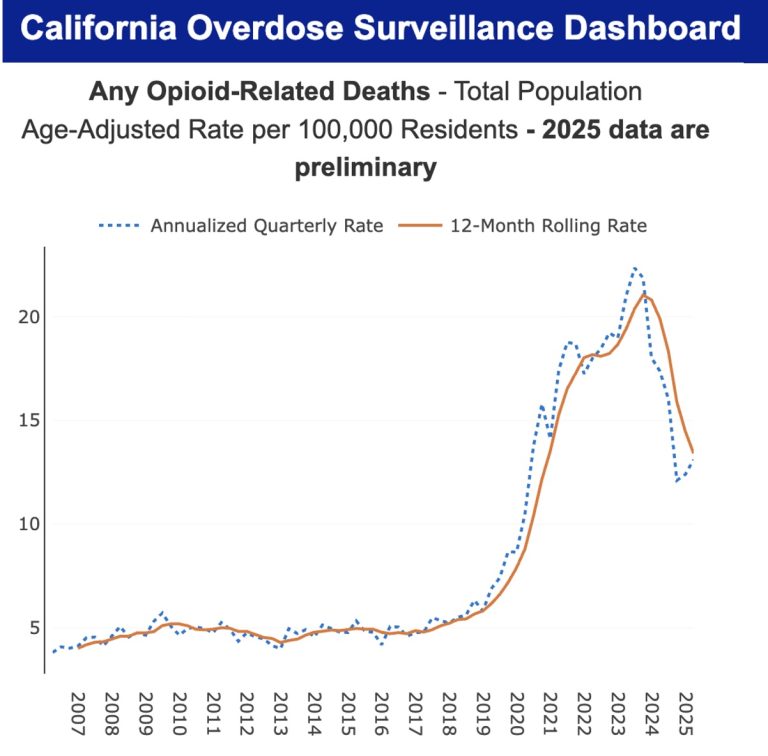
In Stanislaus County, California, fatal opioid overdoses have increased this year, demanding an understanding of why.
Demanding understanding, especially in light of the dramatic drops in that state of fatal opioid overdoses over the past two years, corresponding with even more dramatic distribution of naloxone kits and reported reversals of potentially fatal overdoses (described in detail in the upcoming post:
“OPIOID CRISIS CALIFORNIA: 8 MILLION+ DISTRIBUTED KITS, A HALF MILLION+ DEATHS PREVENTED WITH NALOXONE AS EMERGENCY HARM REDUCTION AGAINST LETHAL EXPERT TREATMENT FAILURE”.
The figures are remarkable, as reported here.
“Since the Naloxone Distribution Project (NDP) began in October 2018, the NDP has distributed more than 7,799,000 kits of naloxone, which have been used to reverse more than 407,500 overdoses.”
As we’ll see in the upcoming post, the increases in saturation and community use of naloxone units far more than account for the approximately 2,400 fewer deaths in 2024/2025.
That raises a critically important question – how, with those levels of statewide naloxone reversals occurring, each one preventing a death, can we understand increases in opioid overdose deaths, as if there are forces so potent continuing to drive high-risk use and overdose, that even those levels cannot keep up.
We, that is, readers at ACD and at Illness and Cure, know the answer to that and how it is hidden, at any cost, including at the cost of a worsening epidemic.
In San Diego County, California, an optimistic headline is belied by the reality of direct reporting from direct service health care providers who know the lives of high-risk users and their behaviors.
And don’t mind saying it plainly, that
“Overdoses are still happening every day. I think that people are just, one, have naloxone and just know how to use it”
That’s what comes through from additional reports from San Diego County, included in this post.
Okay, that makes sense. Because that’s what’s being reported consistently from everywhere, literally everywhere and not just reported by opioid users but also affirmed by data and reports from community workers and others involved in direct service to opioid users.
For example, in San Diego –

There’s a sense of hope on the horizon for people on the frontlines of San Diego County’s opioid epidemic now that the numbers appear to be dropping. Some of that credit is given to getting Narcan in the hands of more people.
A Narcan vending machine is located at the McAlister Institute in Chula Vista. It’s one of at least 16 across San Diego County. These machines are just one of many ways the county and its partners have been working to get the opioid overdose reversal medicine into as many people’s hands as possible.
“It’s one thing to know that there is a magical and lifesaving drug out there, and it’s a different thing to actually be able to access it,” said Marisa Varond, CEO of McAlister Institute, a facility that provides a full continuum of services for people with addictions.
Addiction experts credit access to Narcan for causing a drop in overdose deaths, along with other harm reduction strategies, such as making fentanyl testing strips more widely available and education campaigns, like the billboard that went up in Lakeside. . . .
Tara Stamos-Buseig is effusive in her praise of Narcan’s role. It’s why the Harm Reduction Coalition CEO has also been instrumental in getting more than a dozen Narcan vending machines installed across the county.
But there’s another trend fueled by fentanyl-related deaths that’s caught her attention.
“People are also changing the way they use drugs,” Stamos-Buseig said.
She says that change includes users looking out for each other, ready to administer Narcan, in addition to being more measured in their drug use.
Back to our current post.
“Overdoses are still happening” and are perpetuated by the saturation of communities and communities of high-risk opioid users with naloxone. That’s a worsening crisis and a dead end, unsustainable in light of the emergence of a new opioid crisis more intracatbly lethal with serial overdose reversals and effects of hypoxia, all hidden by deceiving headlines, buried truths, and medical misinformation.
The genesis, shape, and predictable lethal course of an epidemic, whose cause and valid measure of severity – high-risk opioid use and overdose – would be increasingly hidden by confounding effects and unreported use of the life-saving agent naloxone was foreseen, by real reporters.
Real reporters not interested in servitude to the expert class and failed institutions perpetuating the crisis, instead willing to observe and report on the lives of high-risk users on the street. And unafraid of thinking about what they saw and drawing conclusions, as in the “deviant” reporting from 2021 described here.

And in reporting earlier, from 2019, with similar warnings.
And earlier than that, 2018, here at A Critical Discourse.
ADDENDUM:
A worsening opioid crisis appears to be no less difficult to hide in Canada, as exposed in recent posts for provinces Ontario and Alberta, and in this recently appearing, grim news update for locales in Ontario –

An “increasingly toxic and unpredictable” drug supply is driving Ontario’s overdose crisis and has contributed to a recent spike in local opioid overdoses, the health unit says.
Between Feb. 22 and Feb 28, Windsor-Essex emergency departments recorded 19 overdoses, 16 of which involved fentanyl. Local shelters also reported “drastic” increases in the number of overdoses they’ve responded to in recent days.
Another sobering reminder and reality check regarding the dismantled and nullified status of rationales fabricated to mystify the worsening crisis, evidence-free fictions like “supply shock”, disruptions, which cannot escape the incontrovertible fact: the only means by which illicit opioid supply disruptions can have any effect in reducing opioid overdose deaths is by reducing opioid overdoses, which have not been decreasing.
More to come.






