OPIOID CRISIS TRENDS AND THEIR MEANING HELPFULLY OBSCURED IN “EXCLUSIVE” REPORT
The revealing truths that spill into major media reports must be buried by lethal lies, omissions, and thought-free “analysis”
by Clark Miller
Published November 21, 2025
As the grim year 2025 ends, an excited headline trumpets “analysis reveals” the widely different courses of opioid crisis trends across the U.S. that have been apparent for a half-decade or more, widely reported and by necessity their meaning mystified by media/medical consensus and collusion to protect responsible parties from exposure of their worsening epidemic.

But “thought-free”? That’s harsh, isn’t it?
What could lead anyone – so disrespectfully of renowned experts and top investigative media reporting – to come to characterize authoritative, respected media accounts of a lethal crisis with the expert assurances relied on for guidance through the gravest threats to public welfare, as “thought-free”?
Well … there is this and this, and this,
in which the unmoored, remarkably benighted musings and rationalizations of experts, swallowed whole and reported on as meaningful and valid, are deconstructed, nullified as free of supporting evidence, and as contradicted by freely available relevant evidence.
And there is this and this, and this,
in which the weak attempts of America’s medical/media collusion to hide the lethal, failed outcomes of a $344 million opioid gold standard treatment study are revealed as symptomatic of pathological levels of diminished capacity for research literacy, for veracity and integrity, for public duty, for critical thought.
But what about The Guardian’s new, Exclusive Analysis ?
With the provided perspectives of top experts and with graphics so advanced, the analysis must reveal something important and useful. It must, right?
You know, the top experts you’ve trusted over past decades for guidance and response to an increasingly lethal epidemic?

Wow, those are impressive … and what does it mean?
Not to worry, here’s what the Exclusive Analysis reveals, how it helps you understand the mounting deaths and costs of a worsening crisis:
“Public health experts were unsure of what factors led to the decline and whether the reduction in deaths was the beginning of a long-term trend. “You can talk to five different experts, and you’ll get five different explanations for why the deaths are coming down. Nobody really knows”
“We should have much better data on this”
“Of course, that data should be more readily available”
they “may or may not ever know the underlying cause” of a local uptick in overdoses
There is “no clear cause” for the disparity in the statewide data, the spokesperson said.
Kolodny says it is important to understand why deaths are increasing in certain states …That’s hard to tease out.”
That’s not a lot to go on, is it? Not much direction there to assure vulnerable Americans there may be a way out of the worsening, dead-end, epidemic fueled by expert gold standard treatment.
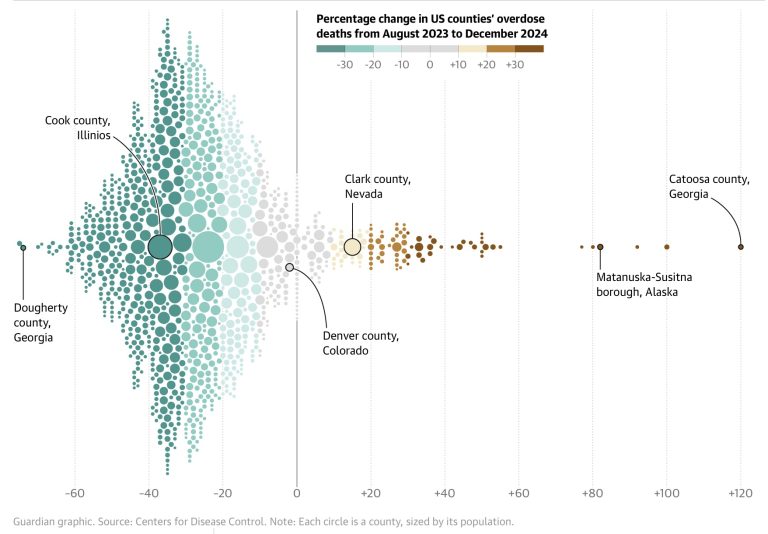
Let’s simplify, starting with an Exclusive graphic that does provide some value.
What is entirely clear is that your benighted experts and science reporters have no idea how to make sense of trends like those.
But we do, and there’s nothing mysterious about it.
All we have to do is look at the wealth of data and evidence for diverse locales, readily available and omitted from The Guardian’s Exclusive Analysis.
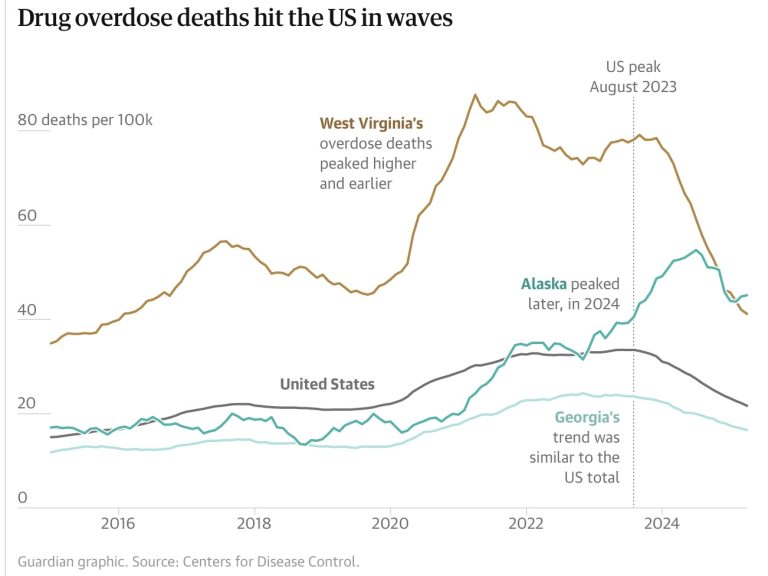
The trend and its causes are clear for West Virginia.

And for Alaska –
But those aren’t the only cases. Instead, consistently in every state and locale examined, the causal relationship holds between timing and effectiveness of naloxone campaigns and drops in incidence of fatal opioid overdoses –
From this previous post –
Let’s repeat that: even as increasingly effective naloxone campaigns are moderating incidence of fatal overdose, the high-risk opioid use desperately necessitating those intensive, nearly nation-wide campaigns is increasing.
It’s the situation not just in Columbus Ohio, but everywhere, evidenced in diverse states, cities and locales across the U.S. consistently, wherever data is available for analysis. Including these locations:
But not in locations that are the exceptions that prove that lethal rule, like Nevada, where lack of effective naloxone distribution and use, along with reckless dispensing of the common street currency for fentanyl (also known as buprenorphine, the “proven” medical cure for opioid use) combine to keep opioid OD deaths mounting. And locations like Iowa and South Dakota, for the same reasons.
The lethal rule is also proven by the exception San Francisco, where an intensive, successful naloxone campaign finally dropped opioid fatal ODs, lagging other locales, followed by opioid deaths now rising again predictably with intensive, publicly-funded dispensing under the direction of medical addiction treatment experts of that common street currency for fentanyl, “bupe, subs”, also in demand for “bridging” or “chipping” to enable fentanyl’s (or heroin’s) episodic use.
That consistency of predictable, naturally replicated results points to the incontrovertible facts that must be escaped and mystified, that no media report dares to say – that all recent drops in opioid overdose deaths are attributable to naloxone campaigns entirely; that high-risk opioid use (and other drug use with associated high risk of opioid overdose) is increasing; that high-risk use (as measured by nonfatal opioid overdose and injection-related infectious disease) is a valid measure of (lack of) effectiveness of American expert gold standard treatments; and that, unavoidably, those treatments are lethal failures.
We might remind ourselves that moderation of high-risk use is the means, and the only means, by which expert gold standard treatments (medication assisted treatment, rehab, and traditional “addiction treatment”) can have beneficial effects.
Back to our current post –
It’s true, naloxone isn’t the entire story. Opioid fatal overdose trends, it turns out, are driven by the combined forces of naloxone campaigns reducing fatalities, while increased provision of America’s expert gold standard treatments – established as fueling high-risk opioid use – drive overdose and fatal overdose upward.
That is established for locales as diverse as San Francisco, Baltimore, Vermont, Nevada, New Mexico, and consistently elsewhere.
Back to the Exclusive Analysis from The Guardian.
It is difficult to tease out how much naloxone has contributed to a reduction in overdose death rates. Evidence is mixed, and the few studies that investigate the impact of naloxone on overdose rates were mostly conducted before overdoses began skyrocketing in the wake of Covid-19.
Those are overt lies, nullified by each of the posts linked to above, starting with –
Boston
Connecticut,
and continuing …
In each, consistently and tightly correlated with fatal opioid overdose trends, data on year-to-year increases (or differences among locales) in actual instances of naloxone used to prevent an overdose from becoming fatal more than account for any and all reductions in fatal opioid ODs for the time frame. And, to repeat, those increases in reversals correlate tightly to time course of trends of reduced opioid overdoses for states and locales, including the exceptions that “prove the rule“.
That holds true when estimates of total reversals are reduced by factors of 5 or 10 (reducing the numbers to 20 or 10 percent of the estimated total) to over-account and compensate for multiple reversals of an individual high-risk opioid user. Read the posts.
Preceding those lies in the Exclusive Analysis are important truths.
Naloxone undoubtedly saves lives, and every public health expert who spoke with the Guardian unequivocally supports its continued promotion. But its necessity is also a grim sign of the severity of the US opioid crisis. Every time someone needed naloxone to reverse an overdose, that person was already on the edge of death – without a friend or bystander with naloxone on hand, their chances of survival would have been slim. People who use opioids encourage one another to “never use alone” and to have naloxone on them at all times.
“It is terrifying,” Fishman said. “I’ve been yelling about this for years. You can’t say I’m gonna reverse an acute overdose and then celebrate when you haven’t addressed the disorder.”
And those truths point intractably, incontrovertiably, lethally, to broader truths, truths so important and clear that they must be hidden, mystified (see for example here and here and here).
Only naloxone campaigns, with consideration of their scale, qualities, effectiveness and timing, are supported by evidence and critical examination as accounting for drops in opioid overdose deaths, and they more than account for the reductions. Those desperate campaigns are required for moderation of the lethal crisis precisely because as driven by established gold standard treatment failure and by all valid, meaningful measures, the crisis is worsening. Worsening because high-risk opioid use continues to surge due to expert treatment failure and because serial emergency naloxone reversals, the only intervention moderating fatalities, are a lethal dead-end.
Those grim facts, as we have just seen, buried by lethal lies, omissions, and thought-free “analysis” in the service of protecting systems of social power and status.






