TRENDING: OPIOID CRISIS FATAL OVERDOSE EXCEPTIONS ARE PROVING THE LETHAL RULE
In another anomalous locale, opioid deaths rise due to lack of naloxone response, exposing the lie of expert cover stories for gold standard treatment failure
by Clark Miller
Published March 13, 2026
Readers who have been following posts at A Critical Discourse or at Illness and Cure will be familiar with that “lethal rule“. (and here). The exceptions are states and locales where, unlike in most of the rest of the U.S., opioid overdose deaths did not begin to drop in late 2023, give or take some months, instead earlier or later.
And those readers will be familiar with the established cause, as illustrated for a rural Washington county in this recent post, of those delays or absence of the significant reductions in overdose deaths occurring in almost all U.S. states over recent years – the failure in those exceptional states or locales to implement the single intervention evidenced as reducing opioid deaths over decades of the crisis, successful campaigns to place overdose-reversing naloxone in the hands of community members proximate to high-risk opioid users.
In Maine, a single county is an exception to all others and an addition to cases consistently proving the lethal rule.

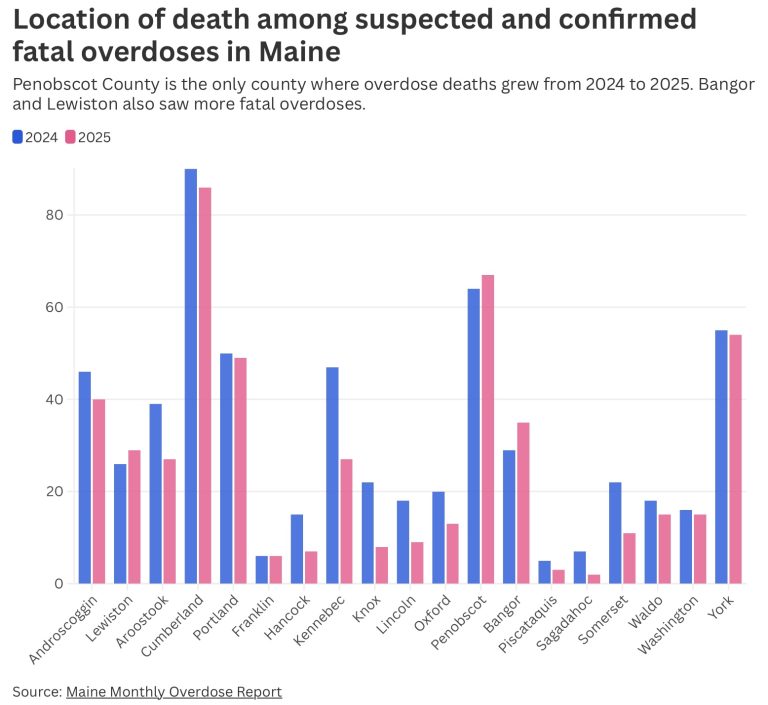
Fatal drug overdoses grew last year in Penobscot County and Bangor despite an overall decline in overdose deaths statewide.
Penobscot County is the only Maine county that saw more suspected and confirmed fatal overdoses in 2025 than the previous year, jumping from 64 to 67, according to a report released this week by the state and University of Maine researchers. That’s 17% of fatal overdoses statewide, for a county that makes up only 11% of the population.
Fatal overdoses statewide declined by more than 20% in that same time, and nonfatal overdoses dropped by 9%.
In 2022, Maine was celebrated by national leaders and experts as a model for the rest of the nation in the effective provision of gold standard medical opioid crisis cures.
Penobscot County and Bangor cannot be considered rural or isolated, and in any case, beginning with COVID adjustments, Maine has adopted relaxed prescribing rules including by telemedicine for buprenorphine, with large increases in dispensing of “bupe’ over past years.
The exceptional increase in opioid overdose deaths in Penobscot County is not about treatment access.
It may, however, be helpful to understand the county’s failure to use funds available for opioid crisis response.
From the same BDN story –
Funds secured through national settlements with companies accused of contributing to the opioid epidemic, which started to be distributed to Maine counties and cities in 2022, could aid efforts to reduce overdose deaths.
Penobscot County had nearly $1.5 million of these funds unspent as of last month, according to a report filed with the state. The city of Bangor has about $650,000 available, all of which an advisory committee plans to distribute to local organizations in the coming week, according to City Manager Carollynn Lear.
That means between those two government bodies, there’s more than $2 million in the bank that could be used to counteract the opioid crisis.
Advocates have criticized the city and county for being slow to spend the money since payments began in 2022. Neither formed an advisory committee to plan spending the funds until last year. Bangor also struggled to quickly spend relief funds meant to counteract effects of the COVID-19 pandemic.
Community direct service providers report “gaps in local harm reduction programs,” including their ability to provide naloxone.
In Bangor, from reports it appears evident that malignant neglect has deprived high-risk opioid users of the access and outreach that in other locales consistently has provided them, their peers, and other proximate laypersons with levels of life-saving naloxone that are established as accounting for the widespread decreases in overdose deaths.
Deprived as in locations that are also exceptions that prove that lethal rule, where overdose deaths did not decrease or increased, while almost all other states saw significant drops. Exceptions like Nevada, where lack of effective naloxone distribution and use, along with reckless dispensing of the common street currency for fentanyl (also known as buprenorphine, the “proven” medical cure for opioid use), combine to keep opioid OD deaths mounting. And locations like Iowa and South Dakota, for the same reasons. And in Alaska and in Washington’s rural Grant County.
As in Nevada and other locales, another potent force in Penobscot County, Maine, contributed to the lethal failure to prevent fatal opioid overdoses.
Associations of high-risk users, including in homeless communities, encampments, or “tent cities”, have increasingly evolved in their members’ use of naloxone that is available to revive each other, by mutual familiarity, proximity, shared values, awareness, and coordination and timing of levels of intoxication for mutual benefit … and survival.
Those protective, life-saving connections are described in some detail in this post and in additional material linked to in that post.
When those ecologies, relationships, and social capital are disrupted, when an encampment is by law enforcement (or otherwise) taken apart, dispersed, it’s members become less protected from fatal overdose, with or without possession of Narcan, until they are able to reestablish reliable connection to others ready to (proximate and cooperative) revive them when needed. When seconds count.
Bangor is one of those locales where those potentially life-saving connections are being disrupted.



As expressed by a Bangor advocate and services provider for those affected by the encampment clearings, reported here, “in order for an overdose to be reversed, the person using drugs has to be around other people”, a truth about social ecologies of illicit opioid use that essentially entirely accounts for drops in fatal overdoses generally and that identifies gold standard expert treatment lethal failure as perpetuating a worsening crisis.
The exceptions confirm a pattern of desperate, emergency naloxone campaigns to moderate lethal effects of failed expert treatments and a worsening crisis – and expose and belie expert cover stories
The example we’ve considered here, along with in this recent post the similar “exception” to general trends in a rural Washington county, should make even more clear the absurdly constructed expert rationalizations for decreases in fatal opioid overdoses including those positing nation-wide or broadly regional effects of high-level changes in supply of or potency of fentanyl reaching the U.S., e.g., fentanyl “market” or “supply” changes, or described as a “nationwide supply shortage” of fentanyl, or “supply shock”, also dismantled here.
In short, across geography, time, and other factors, changes and trends for fatal opioid overdoses comparing regions, states, locales, counties, and cities (as for our example in Maine and for Grant County, Washington) have been the opposite of generalized, instead disparate and remarkably variable, without being remotely consistent with predicted effects of nationwide or even regional changes to drug supply.
Did Grant County, and not any others in Washington, for some reason, escape the “supply shock” affecting the rest of Washington? Did Bangor, Maine, unlike all other locales in Maine?
Was Colorado immune to the nationwide “supply shock” when the “nationwide” supply change was benefiting neighboring states? Were disparate states and locales Alaska, Iowa, South Dakota, San Francisco, Nevada, Tennessee, Utah , and Washington immune too, different somehow inexplicably from proximate states, those exceptions lagging the rest of the nation in fatal opioid overdose drops?
And is it a freakish coincidence that for all of those exceptional states and locales, moreover for states and locales within the general pattern and those outside it, the timing and effectiveness of naloxone campaigns in each case are correlated tightly with the drops in opioid deaths?
That’s something that would require a trusted, top expert to explain, and a professional class of compromised useful idiots to convey to a vulnerable public.
Exceptions that are not exceptions,
that are not a “puzzle“, instead point clearly to a worsening epidemic, must be buried, covered up with fabrications. Desperate, unsustainable Narcan campaigns that revive high-risk opioid users – to use again, and again – are hiding the persistent worsening of high-risk opioid use, a valid measure of lethal failure of gold standard treatments.
My take on X –
Risk of exposure of expert and institutional culpability for lethal epidemics
demands desperately, recklessly fabricated lies.
THE “SUPPLY SHOCK” DECEPTION IS INVALIDATED BECAUSE
1) CONSISTENTLY FOR ALL LOCATIONS, THOSE DROPS HAVE ALREADY BEEN ACCOUNTED FOR BY ESTABLISHED YEAR-OVER-YEAR DRAMATIC INCREASES IN NALOXONE REVERSALS OF OTHERWISE FATAL ODs
Those Narcan reversals happened, can’t be undone, or erased, leaving no OD death drops to be accounted for by other hypothesized factors, including supply quality.
2) among widely differing states and locales, opioid death rate trends varied wildly, NOT in broad, uniform ways as predicted by national supply changes across the U.S.,
including between proximate states and locales (described in detail here ), with no apparent patterns that are consistent with supply changes.
The patterns instead are established as consistent with variations in timing and effectiveness of naloxone campaigns among states and locales

A third, independently nullifying outcome follows from the incontrovertible fact that for a “supply shock” or any supply disruption factor to affect opioid overdose deaths, that disruption MUST REDUCE PREVALENCE OF HIGH-RISK OPIOID USE.
High-risk opioid use and overdose are increasing, everywhere, in a worsening crisis, by all valid measures.






